Introduction
The US health care system is characterized by complexity, fragmentation, and suboptimal coordination, posing significant challenges to achieving optimal patient outcomes and controlling health care costs.1 The presence of multiple payors, fragmented financing, and outdated reimbursement processes exacerbates these challenges, hindering innovation and collaboration among diverse health care professions and organizations.2,3 Consequently, there is a pressing need for adoption of blended payment systems that incentivize collaborative, patient-centered care within interprofessional teams.1,4,5
Moreover, the US health care system is widely recognized for its exorbitant costs, complicated structure, and comparatively lower quality when compared to other developed nations.6 The disjointed nature of the system, coupled with its reliance on traditional fee-for-service (FFS) payment models, conceals its progress toward improved health care outcomes by hindering care coordination and investments in health information technology infrastructure while prioritizing volume of services over value-based care delivery. With escalating costs, restricted access, and persistent quality issues, urgent reforms are imperative to enhancing health care delivery and outcomes nationwide.1
The challenges confronting the US health care system, including high-cost, low-quality health care services and outcomes, are not unique and echo those seen in high-performing systems worldwide. However, what sets high-performing systems apart is their ability to transform these challenges into opportunities for positive change.
In 2019, the US health care system’s average cost per person was almost two and a half times the average of 35 OECD countries.6 Despite the high health expenditures, the United States lags behind in key metrics such as life expectancy, access to care, and quality of care.6 The health care system also faces a myriad of challenges, including an aging population with multiple chronic diseases, widening health disparities, the impacts of climate change, repercussions from pandemics, global socioeconomic instability, and large-scale migration, placing significant strains on health care resources.7 Fragmentation and a lack of collaboration and coordination across health care professions and agencies are identified as primary reasons for the high cost and low quality in the health care system.2,8
To address current and future challenges, immediate reforms within the health care system are imperative.7,9 In response, interprofessional team-based care emerges as a pivotal strategy to enhance patient outcomes and optimize service delivery efficiency, especially in managing chronic diseases and transitioning to value-based care models.8,10,11 The aim is to harness the diverse skills and expertise of various health care providers within their full scope of practice, without introducing unnecessary specialization that could lead to care fragmentation. Through this approach, team-based care seeks to boost efficiency and effectiveness, expand access, and elevate satisfaction for all stakeholders, including health care providers and patients.1
Financial incentives, as a determinant of clinicians’ decisions, significantly impact the volume and nature of care services provided.12,13 Clinicians may be inclined to prioritize services with higher financial returns, potentially influencing the utilization and composition of health care services. The disproportionately low allocation and valuation of total health care expenditures to team-based care and primary care—with rates paid for primary health care being lower than those paid for specialty or procedural care—intensifies challenges in retaining experienced primary health care clinicians, a situation further exacerbated by the strains of the COVID-19 pandemic, which led to the closure of many primary health care practices.5,10,14
It is important to distinguish between primary care and primary health care. Primary care refers to the initial point of contact with the health care system, typically provided by general practitioners, family physicians, or pediatricians. On the other hand, primary health care encompasses a broader range of health care providers, services, functions, and goals, including health promotion, disease prevention, treatment, rehabilitation, and palliative care.5
We need a health care system that places greater emphasis on interprofessional team-based care, aiming to foster a healthier population with consistent access to primary care services and a potentially more equitable distribution of health care resources.1,15–17 Payment methods in health care significantly shape clinician behavior, with fee-for-service models often incentivizing a focus on individual billable services at the expense of non-billable services that contribute to positive health outcomes.
In light of these formidable challenges, this paper aims to delve into payment models specifically tailored to interprofessional team-based care. Recognizing the pivotal role of payment models in shaping the future of health care delivery in the United States, this exploration seeks to offer insights and recommendations for policymakers, practitioners, and educators striving for a health care system that prioritizes collaboration, patient-centeredness, quality, and sustainability.
Background
The transition from fee-for-service to value-based care represents a pivotal mechanism in unlocking the full potential of interprofessional team-based care to shift the burden of risk from patients/payors to health care providers.14,18,19 By fostering cross-professional and inter-agency collaboration, value-based payment models incentivize providers to prioritize patient-centered care and improve overall service quality and health outcomes. The reactive and transactional nature of fee-for-service is ill-suited to the collaborative and proactive approach inherent in interprofessional team-based care, often constraining providers by time limitations.1,19
Value-based payment models emerge as catalysts for innovation, fundamentally redefining health care delivery by prioritizing quality and outcomes over the sheer volume of appointments.20 This paradigm shift allows care to extend beyond traditional office hours, leveraging interprofessional teams and technological advancements to provide comprehensive patient support. Moreover, it acknowledges and rewards the care coordination and collaborative management efforts of health care teams, aligning incentives with proactive patient engagement. Empowering health care providers to build meaningful relationships with patients fosters trust and rapport, leading to more effective health management, earlier detection and intervention, and ultimately improved patient wellness and population health.18,20
For this transformative shift to succeed, policymakers must accelerate the adoption of value-based payment models across broader patient populations and health care settings. Legal frameworks play a crucial role in shaping payment models, and policymakers must address regulatory barriers to effective interprofessional collaboration. Advocating for supportive policies that align with the goals of interprofessional team-based care is essential, ensuring legal frameworks facilitate successful implementation within various payment models.2,14,20
Furthermore, policymakers should prioritize the development of regulations that incentivize and support the adoption of payment models conducive to interprofessional collaboration. This includes addressing reimbursement structures and providing frameworks that encourage the integration of diverse health care professionals in team-based care. By proactively addressing these issues, policymakers can pave the way for a more collaborative and effective health care system that prioritizes patient-centered care and enhances overall health outcomes.
Health Care Payment Models
Health care payment models for interprofessional team-based care have been developed to provide high-quality care to patients while improving cost-effectiveness. These models incentivize health care providers to work together to provide coordinated care to patients. Here is an overview of the common payment models and the way they foster (or hinder) achievement of this goal.
Fee for Service (FFS)
FFS, a traditional payment model, operates by reimbursing health care providers based on individual services rendered. While this approach incentivizes volume, it also presents challenges to interprofessional collaboration due to its reliance on itemized billing. Furthermore, the model may not align seamlessly with patient-centered goals, potentially leading to fragmented care. Numerous studies have highlighted the drawbacks of FFS, including its association with overutilization of services and a lack of focus on preventive care, indicating the need for a shift toward more collaborative payment models.2,5,14,20–22
Capitation
Capitation involves paying a fixed amount per enrolled patient to health care providers. This model encourages preventive care and population health management, fostering collaboration among diverse providers. The focus on overall patient well-being and predictable costs for health care systems adds to its appeal as a viable payment model. Research has shown that capitation models are associated with improved preventive care measures, leading to better overall health outcomes for patients, making capitation a valuable consideration for interprofessional team-based care.2,5,21,23
Pay-for-Performance (P4P)
P4P programs typically involve financial incentives or penalties based on the achievement of predefined performance measures. Providers receive bonuses or face reductions in reimbursement based on their performance in meeting quality metrics, such as patient outcomes, adherence to clinical guidelines, or patient satisfaction scores. P4P aims to incentivize providers to deliver high-quality care and achieve better outcomes. P4P programs in health care have consistently shown improvements in the quality of care, including better adherence to clinical guidelines, increased rates of preventive services, and reductions in hospital readmissions and complications. Moreover, P4P incentives have been associated with positive changes in provider behavior, such as the adoption of evidence-based practices and care coordination efforts.5,14,21,24–26
Value-Based Care (VBC)
VBC is a broader concept that encompasses various payment models and approaches aimed at aligning reimbursement with the value of care delivered. Unlike traditional FFS models that reimburse based on the volume of services provided, VBC models focus on the quality, outcomes, and cost-effectiveness of care. These models often include P4P components but may also incorporate other elements such as capitation, shared savings, or global payments. VBC models have shown promise in improving patient outcomes, health equity, and reducing unnecessary health care costs, underscoring their potential as an effective payment model for fostering collaboration among interprofessional teams.5,14,24,27
Bundled Payments
Bundled payments offer a fixed price for an entire episode of care, such as joint replacement. This model promotes collaboration among health care teams spanning different specialties, working together to optimize outcomes. However, successful implementation requires clear care pathways and a delicate balance of cost containment with maintaining high-quality care. Studies have demonstrated that bundled payments can lead to cost savings and improved coordination among health care providers, emphasizing the potential benefits of this model in fostering interprofessional collaboration.14,24,28,29
Accountable Care Organizations (ACOs) and Shared Savings
ACOs are groups of health care providers that work together to provide coordinated care to patients, while shared savings is a payment model that rewards health care providers for reducing costs while maintaining quality. Both ACOs and shared savings incentivize providers to work together to provide high-quality care and reduce health care costs. ACOs and shared savings have been shown to improve the quality of care, reduce costs, and promote collaboration among health care providers, making them effective models for interprofessional team-based care.14,28,30–32
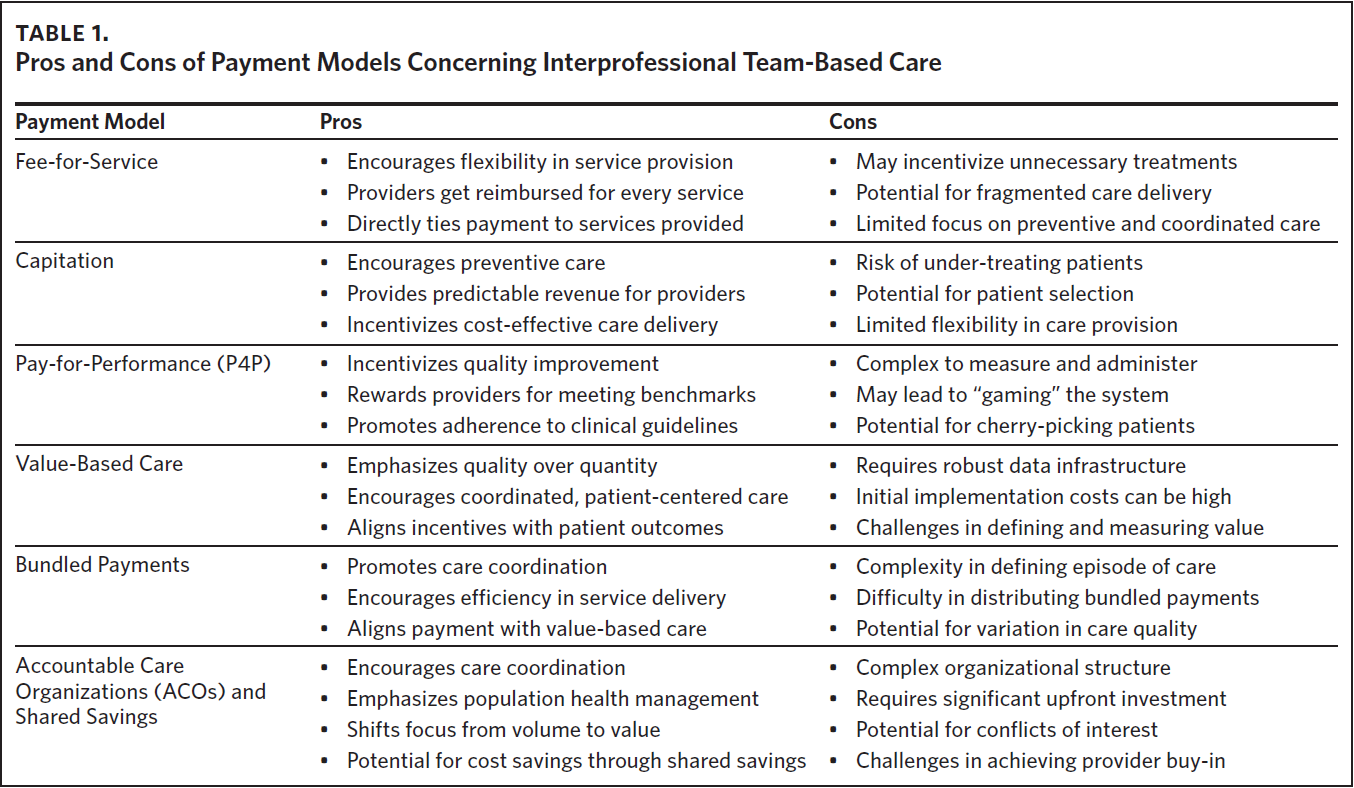
In summary and as outlined in Table 1, health care payment models play a critical role in fostering (or hindering) collaboration among interprofessional teams and delivering high-quality, cost-effective care to patients. By aligning financial incentives with patient outcomes and quality metrics, these models incentivize providers to work together to achieve common goals and improve the overall delivery of health care services.

Discussion
Navigating the complexities of health care transformation necessitates a deep understanding of how payment models impact interprofessional teams. By integrating evidence-based practices and innovative approaches, this review serves as a guide for stakeholders committed to shaping a health care system that prioritizes efficiency, quality, and sustainability. Through collaborative efforts among policymakers, practitioners, and educators, we can pave the way toward a future characterized by patient-centered, interprofessional health care delivery.
The discussion about payment methods highlights their distinct impacts on clinician behavior, from fee-for-service to bundled payments. Concerns about under-provision of care often arise when clinicians bear financial risk, whereas fee-for-service models may lead to over-treatment. Empirical findings support these theoretical expectations, with fee-for-service models encouraging higher service utilization and capitation models discouraging unnecessary resource consumption.14 Blended payment approaches that combine capitation (or the fee for service) with value-based payment model elements show promise in supporting high-quality primary health care and optimizing incentives for better patient outcomes. Moreover, evidence suggests that hybrid payment models can mitigate fee-for-service model shortcomings, promoting care quality and efficiency in the long run rather than serving as a short-term cost reduction mechanism.
The health care industry is transitioning toward value-based contracts to lower costs and deliver proactive primary health care. While discussions often focus on a complete shift from fee-for-service, a hybrid payment model is gaining traction. The National Academies of Sciences, Engineering, and Medicine1 recommend a hybrid payment model for primary health care and interprofessional team-based care, blending capitation (or the fee for service) and value-based contracting. This approach allows health care organizations to adopt alternative incentive programs without compromising financial stability. The hybrid model emphasizes advanced primary health care and interprofessional team-based care, focusing on person- and family-centered, high-value, team-based, accessible, and coordinated care attributes.18,19
Health care payment model reform should be regarded as an investment in future health asset capacity and equity production, rather than an immediate solution for reducing health care costs.14 Evidence indicates that payment reform alone may not decrease total costs of care in the short or medium term.5 However, incorporating interprofessional team-based care with robust value-based payment models can lead to long-term efficiency and effectiveness, particularly in chronic care management and health equity.4,10 Strengthening interprofessional team-based care can significantly reduce health care costs and improve care quality by decreasing ambulatory care, emergency room visits, and hospitalizations.1,23 System-wide changes are necessary to orient the health care workforce and practice patterns toward interprofessional team-based care delivery and primary health care for sustainable transformation in the health care system in the United States.1,19,20,33
Conclusion
In the dynamic landscape of health care, the way we pay for services profoundly influences how care is delivered, experienced, and coordinated. Interprofessional team-based care, which emphasizes collaboration among diverse health care professionals, has gained prominence as a means of improving patient outcomes, enhancing quality, and optimizing resource utilization. However, the alignment of payment models with interprofessional practice remains a critical area of exploration. Health care payment models play a critical role in shaping how health care services are funded, delivered, and experienced by patients. These models impact provider behavior, patient outcomes, and overall system sustainability.
In conclusion, the introduction of various value-based payment models within primary and specialty care reflects ongoing efforts to transform health care delivery and improve patient outcomes. These models incorporate diverse approaches, including multi-payer reforms, home-based care, collaborative learning networks, and bundled payments. The hybrid payment model for interprofessional team-based care and primary health care represents a versatile approach, offering a balance between capitation (or the fee for service) and value-based contracting to support the transition toward more efficient and patient-centered care. We need a payment model that supports sustainable, team- and relationship-based, high-quality, integrated primary health care, aiming to ensure ready access to primary health care teams across modalities and address social determinants of health (SDOH). Highlighting the need for adequate payment to support primary health care practices and accommodate emerging delivery models, payment reform should be viewed as an investment in improving patient/population health rather than as a mechanism for significant short-term cost reduction.
Acknowledgments
The author reports no potential conflicts of interest.