Introduction
In North Carolina, 87 out of 100 counties have a primary care provider shortage, while 90 lack mental health providers and 76 lack dental health resources.1 The reasons for this workforce gap are multifaceted and complex, and lack of education about and exposure to rural experiences make it difficult to recruit health care professions graduates to rural communities. Best practices include exposing students to longitudinal experiences in rural communities with the goal of having them return to these communities upon graduation to provide enhanced health care. These experiences also create opportunities for current health care professionals to develop skills of mentorship and preceptorship, creating a mechanism for leaders to retain and support the next generation.
Due to generous support from the William R. Kenan, Jr., Charitable Trust, the UNC Rural Interprofessional Health Initiative (RIPHI) began in 2017 as a partnership between the Office of Rural Initiatives in the University of North Carolina at Chapel Hill (UNC-CH) School of Medicine and faculty within the UNC health professions schools. Funding has supported several iterations of the RIPHI model since 2017, and it has had several evolutions and modifications as it has evolved. RIPHI aimed to address increasing rural workforce needs in North Carolina through interprofessional collaboration opportunities in rural communities, where health care professionals and students work as a team to implement population-based interventions to improve care. The initiative provides the infrastructure to engage students in rural interprofessional health initiatives through exposure to rural health through classroom activities, presentations, events, and intentional interprofessional immersive experiences. In June 2023, RIPHI received the Excellence in Interprofessional Education Collaboration Award from the Interprofessional Education Collaborative.2
In 2017, RIPHI began as an elective opportunity in which interprofessional students from the health professions schools completed a three-credit-hour course focused on interprofessional population health. Faculty from the health professions schools (RIPHI champions) served as mentors during the course. Students completed online modules addressing population health concepts and then came together twice a month to develop a solution to a hypothetical population health scenario in a rural setting. They presented their solution to the RIPHI champions at the end of the semester. This experience was designed to prepare them for the next semester, when teams were partnered with real rural communities where they worked alongside local health care professionals and community organizers, as well as the RIPHI champions, to apply quality-improvement principles to population-based clinical needs.
As part of the original 2017 award, RIPHI hosted three rural symposia with leaders across the state, including North Carolina Area Health Education Centers (NC AHEC), that formed a collaborative to address rural health issues. During the February 2020 symposium it was suggested that the model be revised to 1) expose more students to rural health activities to increase their understanding of the needs of rural communities (EXPOSURE) and 2) intentionally focus efforts for a cohort of students who have a specific passion for rural health (ENGAGEMENT). In 2023, a third aim was added (TRANSFORM) that focuses on intentional partnership with community practices to provide a formative assessment and support their ability to be collaborative-practice ready.
Interprofessional Team Exposure to Rural Health Needs
With the creation of a formal interprofessional office in 2018, RIPHI is housed under the Office of Interprofessional Education and Practice (IPEP) at UNC-CH. This infrastructure supported the first aim of RIPHI by transitioning it from a successful population health elective to a required educational opportunity for all health professions students. This activity is now embedded as part of coursework in partnership health professional schools and departments. Faculty from each partnering school collaborated to design, deliver, and evaluate the content of the “Partnership for Population Health” series (P4P), which has been continuously offered since Fall 2020, serving 300 to 700 students per semester. Students complete learning modules on population health topics using a competency-based evaluation system. Students are placed in virtual interprofessional teams to work through a three-part unfolding case based in a hypothetical community health center in a real North Carolina county. In 2022, RIPHI launched a more engaging format for the embedded case activity in which students on interprofessional teams use an avatar-based platform to design an interprofessional population health intervention addressing teenage vaping in a rural county. Since 2018, over 4,000 students have participated in this interprofessional classroom activity.
Engaging with Rural Communities
The second and third aims of RIPHI (ENGAGE and TRANSFORM) focus on intentional partnership with rural community partners. The Rural Interprofessional Longitudinal Scholars (RIPLS) Program began in 2021 as a pilot modeled after components of the Kenan Primary Care Medical Scholars Program in the Office of Rural Initiatives. RIPLS students participate in monthly seminars on rural health and interprofessional practice and complete a six-week immersion experience in which they partner with a real rural community to produce a high-impact project. Students also receive tuition support during their time as RIPLS. Projects are designed with the community partner and can be assessment- or intervention-focused. Since initial funding, over 150 students have engaged with nine rural communities. Each project is unique, with different outcomes depending on the population served. A few examples include increasing aspirin and statin use for individuals with diabetes in a rural primary care clinic, identifying super-utilizers in a home health setting, connecting resources to address social determinants of health in a rural emergency department, increasing self-efficacy for diabetic patients, and completing asset mapping for a “lifestyle is medicine” program.
In 2023, RIPHI received additional funding to expand the RIPLS model beyond UNC-CH students and to develop infrastructure to maintain longer relationships with communities. A RIPHI champion was identified by our partners at UNC-Wilmington. This individual is a staff member who serves as the main contact for students and community partners in the local area. This individual works closely with South East Area Health Education Centers (SEAHEC) to identify practice partners and existing infrastructure to maintain sustainability of the work. Eight UNC-CH students from the disciplines of occupational therapy, dentistry, speech and hearing, public health, and social work partnered with three UNC-Wilmington students from public health to complete a needs assessment of Pender County in partnership with a rural primary care clinic. Students visited primary care locations, restaurants, places of worship, gas stations, and community centers to ask residents about their top health needs. This information was combined with public health needs assessment data and workforce projections to make recommendations for health care provider recruitment. The top health needs identified focused on mental health, oral health and diabetes, and the need for materials addressing health literacy. In partnership with the primary care clinic, students from both universities will work collaboratively across professions to develop resource materials for community members at the local community center. Results from the health fair will inform the activities of the 2024 summer immersion experience for the next cohort of RIPLS from UNC-CH and UNC-Wilmington. This next cohort will include eight students from each institution. In 2025, the model will be expanded with a third university partner.
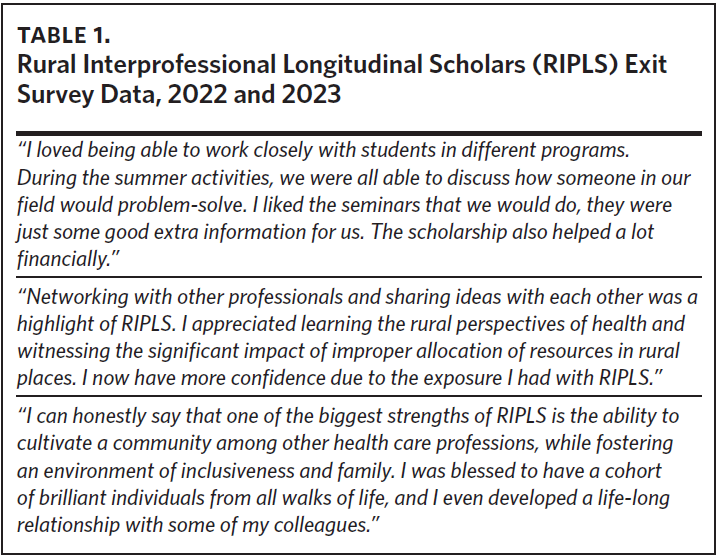
Results from the RIPLS program have been positive. Since RIPLS transitioned to a more intentional scholarship program in 2019, 24 students from UNC-CH have completed it and all have gone on to care for rural patients, either through direct practice in a rural community or working with policymakers and designing interventions for rural health. Two are currently pursuing additional graduate degrees in their profession (nursing and social work) to focus on addressing social determinants of health for underrepresented populations. Exit survey data from the 2022 and 2023 cohort support the hypothesis that a cohort-based model reinforces the value of interprofessional collaboration and builds self-efficacy to practice in a rural community (Table 1). Tuition has often been a barrier to pursuing advanced degrees, and the RIPLS model provides tuition support while in school, rather than a loan repayment model.

Looking Ahead: Building Sustainability
The final aim of RIPHI (TRANSFORM) is in progress and focuses on building up mentorship and site development of current practices in rural communities through partnerships with NC AHEC and other entities. Practice and site development are essential for sustainability and measurement of impact on patients and the rural communities themselves. Building up interprofessional sites will allow students to develop relationships with mentors that can support them beyond their time in a health professions program and create a culture of collaboration that empowers practitioners in rural communities. For this goal, practices will use the IP-CLEAR Tool to identify strengths and gaps in interprofessional practice. Site and leadership development resources created by the Interprofessional Education Leaders Collaborative (IPELC) and Relational Leadership at Carolina will be used based on identified needs. Mentorship programs for preceptors and other resources needed by the site will be provided.
As the health inequality gap between rural and urban communities continues to widen, health care workers in under-resourced communities must learn to deliver health care through a collaborative lens. In other words, interprofessional practice is essential for the future health of North Carolina, and we need more interprofessional opportunities for students to engage and learn from, with, and about each other in order to improve health outcomes. The RIPHI model provides exposure, engagement, and transformation, creating a culture in which clinicians desire to practice, and mentorship support to help them thrive.
For sites wishing to replicate this model, RIPHI offers a few lessons learned and tips for success. This work is complex and has many parties and communities to engage. Faculty partners, students, community members, practice sites, and large health organizations all have different goals. With often competing demands, it is important to remember that the ultimate goal is to intentionally and collaboratively develop interventions that benefit patients and populations. When decisions about next steps become difficult, remind teammates of this overarching goal. It is essential to build and sustain relationships; when multiple parties engage to do work like this, community members must be at the center and be supported for their time as much as possible. Check in frequently with team members through regular meetings and email communications to make sure that all have the same goals in mind. When conflict or confusion arises, it should be addressed quickly and in person as much as possible.
The most important recommendation is to start with a pilot. Building infrastructure for interprofessional education and practice takes time; schools and departments often have different policies regarding students, schedules are different, and student rotations can vary. These are often seen as barriers to implementation of interprofessional education and practice and can stop a project before it begins. Pilot work can help build momentum and engagement and help problem-solve on a smaller, more manageable level. Embracing a continuous quality-improvement mindset will help to further refine the work and the ability to disseminate the model to multiple communities. To learn more about the Rural Interprofessional Health Initiative or to partner with us, visit https://ipep.unc.edu.
Acknowledgments
The authors would like to acknowledge the support of the William R. Kenan, Jr. Charitable Trust, as this funding has made this work possible. To the many champions of rural health in our academic and rural communities—we appreciate your partnership.
The authors reported no conflicts of interest.