Introduction
We often think of US health care crises as those making headline news: pandemics, the spreading of vaccine-preventable diseases, or the loss of vital insurance coverage. A quieter but equally consequential emergency is unfolding: the widespread closure of community pharmacies. This trend is eroding a critical access point for health care—especially in rural and underserved areas of North Carolina—and demands immediate attention.
Beyond their familiar role of dispensing prescription and over-the-counter (OTC) medications, pharmacists practicing today in community pharmacy settings (chain, independent, free clinics, and health department operations) provide a variety of vital diagnostic-, preventative-, and treatment-related health care services. These include health screening, disease prevention and medication-related patient education/counseling. To supplement their required education, many pharmacists carry additional training and/or certifications (including designation as a certified pharmacy practitioner), which enable provision of services such as smoking cessation, diabetes, hypertension, hyperlipidemia, asthma, HIV management, and access to hormonal birth control for eligible patients. In addition, pharmacists provide vital immunization services. As an example, member partners of the Federal Retail Pharmacy Program administered 40.5 million (67.7%) of the COVID-19 bivalent vaccine doses administered in the United States from September 1, 2022–September 30, 2023.1
Community pharmacists provide ready and vital access to health care services, often to populations unwilling or unable to use traditional primary health care practitioners. In one study, researchers found that 73.1% of the US population lived within 2 miles of a pharmacy, and 88.9% within 5 miles.2 Patients visit their community pharmacies almost twice as often as they visit their physicians or other qualified health care providers.3 In all 50 states and in all but 9 US counties, the number of community pharmacy visits among these Medicare beneficiaries was larger than the number of encounters with primary care physicians.4 Here in North Carolina, 1770 of 2352 (75.26%) pharmacies operate within either a Medically Unserved Area/Population (MUA/P) or a Health Professional Shortage Area (HPSA).5
Community Pharmacy Closures
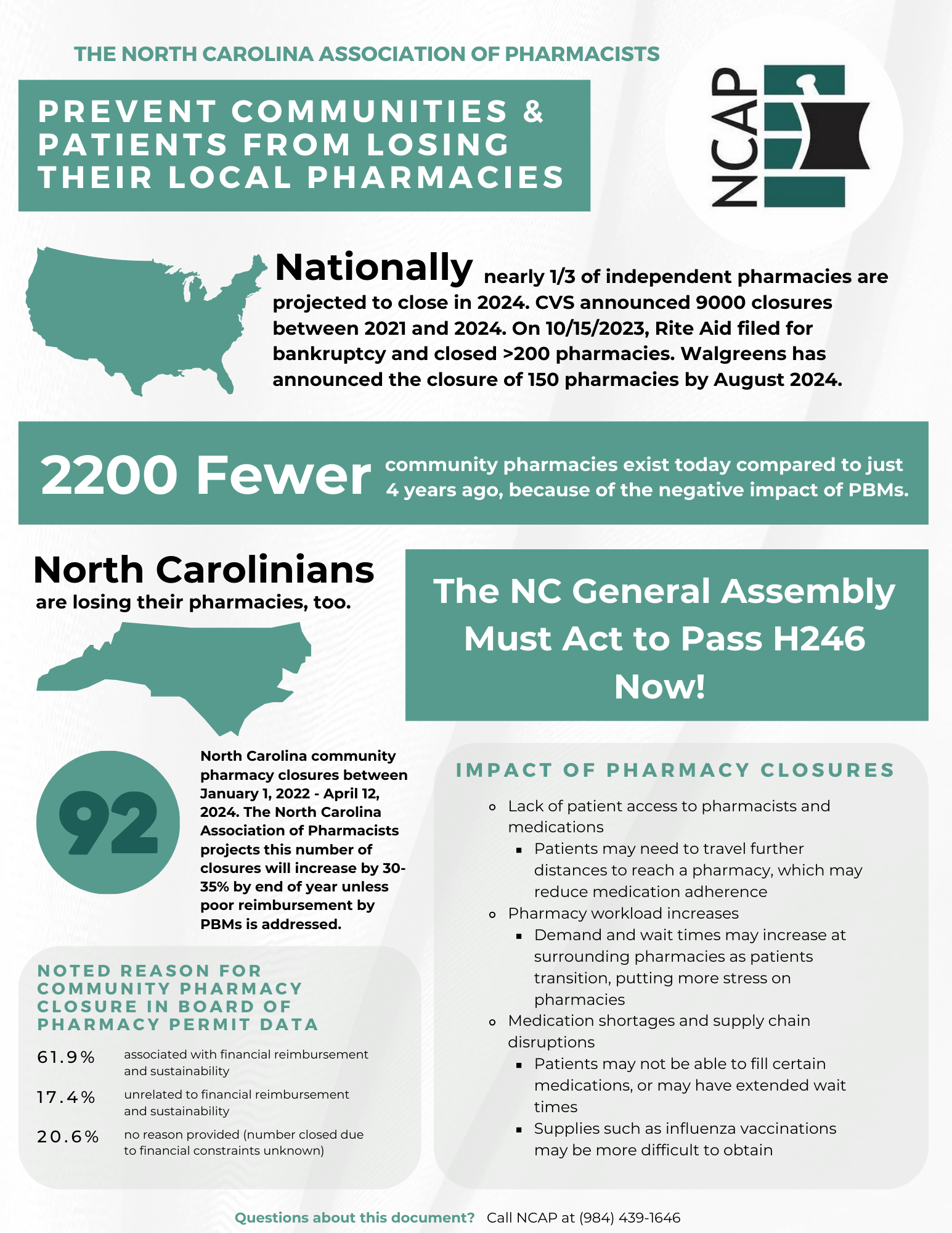
Despite their essential role in health care delivery, community pharmacies are closing at an alarming rate across the United States. Between 2018 and 2021, more pharmacies closed than opened, with 41 states experiencing a net loss.6 These closures disproportionately affect independent pharmacies and those located in Black, Latinx, and rural communities.6–8
Approximately 15 million Americans (or about 5% of the population) depend on independent pharmacies for primary health care access.9 These individuals are more likely to be older, live in rural areas, and belong to low-income households.9 Independent pharmacies (specifically in both rural and urban areas serving lower-income, uninsured, or publicly insured populations) were more likely to close than their chain pharmacy counterparts.6 Looking ahead, a survey conducted by the National Community Pharmacists Association (NCPA) reported that closure rates of 20%–25% are anticipated in the coming year.10 Chain pharmacies are also scaling back. Rite Aid has closed over 300 stores amid bankruptcy proceedings, with more closures expected. CVS and Walgreens have announced plans to shutter hundreds of locations, with urban areas likely to feel the greatest impact due to the higher concentration of chain pharmacies in these regions.2
Available data on the closure of North Carolina community pharmacies are also alarming. Between January 1, 2021, and June 5, 2025, licensure data obtained from the North Carolina Board of Pharmacy (NCBOP) listed 210 closures of community operations (as indicated by a previous active license transitioned to inactive license operating as independent, chain, free clinic, or health department with a primary address within North Carolina). While the number of closures does not address the impact of new operations offsetting these closures, the amount and rate of closures is significant, nonetheless. Such rates of closure are likely to continue or worsen. The North Carolina Association of Pharmacists predicted the rate could increase to 30%–35% without intervention.11
Areas without community pharmacy access are often characterized as “pharmacy deserts.” Modeled after the term “food desert” (reflecting a lack of access to food), it is intended to characterize a community where residents are required to travel farther to the nearest pharmacy. Criteria used to determine such a designation vary between studies, and critics cite several limitations that may oversimplify or misrepresent health care access. Despite the limitations, studies characterizing pharmacy deserts help illustrate area differences in pharmacy access and its impact. In one report, 8.3% of US counties had at least 50% of residents living more than 10 miles from the nearest pharmacy.2 In North Carolina, 17.2% of urban areas (1.3 million residents) and 4.25% of rural areas (140,000 residents) were identified as pharmacy deserts.12 Areas with the highest density of pharmacy deserts also exhibit high indices of social vulnerability.13
The Reasons are Complex
The accelerating rate of community pharmacy closures is driven by an interplay of economic, regulatory, and workforce-related factors. While consolidation and the closure of underperforming chain pharmacy locations contribute, deeper systemic issues are also contributing to the decline.
Workforce Challenges and Market Competition
Recruiting pharmacists to rural areas remains a persistent challenge. Community pharmacists note higher rates of excessive workload and reduced job satisfaction relative to their counterparts in other work settings.14 Simultaneously, competition from non-traditional providers (such as Amazon and other online pharmacies) has disrupted the traditional pharmacy model, drawing patients away from local operations.
Reimbursement Pressures and Delayed Payments
Community pharmacies, particularly those serving publicly insured or low-income populations, face shrinking reimbursement rates from Medicare and Medicaid. Payment delays further strain cash flow, making it difficult for small, independent pharmacies to remain solvent.
The Role of Pharmacy Benefit Managers (PBMs)
PBMs are organizations that serve as intermediaries between insurers, pharmacies, and drug manufacturers, managing formularies, negotiating prices, and processing claims. According to the Federal Trade Commission (FTC), 4 companies control over 70% of the PBM market, with the top 3 companies managing 80% of all US prescriptions.15 Many PBMs operate their own mail-order or specialty pharmacies, creating potential for conflicts of interest that further disadvantage unaffiliated community pharmacies. PBMs may reimburse community pharmacies at rates below the cost of acquisition and dispensing. Additionally, they may charge health plans more than they reimburse pharmacies. Direct and indirect remuneration (DIR) fees often lack transparency, further eroding pharmacy margins (especially for independent operations).16
Network Exclusion and Disparities
Pharmacies in minority and low-income neighborhoods are more likely to be excluded from preferred networks, increasing out-of-pocket costs for patients and reducing pharmacy revenue. Since Medicare Part D accounts for roughly one-third of national prescription drug spending, exclusion from these networks can be financially devastating.16 DIR fees, originally intended to adjust payments based on performance, are now applied broadly and are often based on metrics outside a pharmacy’s control (such as patient adherence or generic dispensing rates), which further penalizes community pharmacies.
A Call to Action
Given the complex nature of community pharmacy closures, no single intervention will likely be sufficient. Therefore, a comprehensive, multifaceted strategy is essential; one that includes both immediate relief and long-term transformation of community pharmacy service delivery.
Promotion of Community Pharmacy Practice
In their article titled “Act for the Future of Community Pharmacy,” Bacci and colleagues share their vision of a patient-centered community pharmacy practice of the patient’s choosing that provides equitable access to expert and valued integrated care.17 In support of this vision, they call for engagement with and recognition of the role and value of our community pharmacist colleagues in a team-based approach to patient care, and enhanced collaboration with pharmacy colleagues. In addition, they advocate for improved workplace environments and increased educational opportunities for pharmacists wishing to pursue community pharmacy practice. Furthermore, they call on the pharmacy community to advocate for community pharmacy payment transparency and transformation, as well as enhanced awareness of the impact of these closures on the health of the community they serve.
Innovative Service Models
For areas presently underserved, alternative pharmacy service delivery models may provide some relief. Mail-order pharmacies would enable patients to order their prescriptions online and have them delivered to their homes without need for patient transportation. One example currently in use is NC MedAssist, which allows patients to receive medications at home, reducing transportation barriers.18 Telepharmacy has shown comparable quality to traditional models but faces regulatory hurdles in some states.19
Legislative and Regulatory Reform
Federal and state-level reforms are critical to address systemic inequities. The stalled Pharmacists Fight Back Act (H.R. 9096) sought to regulate PBMs. Efforts to reform regulations governing PBM operations through legislative reforms have also been undertaken in several states. Areas addressed include (but are not limited to) PBM operations, drug pricing, transparency, reimbursement, cost-sharing, and prior authorization.20 In North Carolina, the North Carolina Association of Pharmacists (NCAP), among other stakeholders, works with state lawmakers advocating for payment for pharmacy clinical (non-dispensing) services and PBM reform. The results of such advocacy are reflected in pending legislation. North Carolina House Bill 163 (HB 163) aims to provide oversite and regulation for PBMs, improve transparency, eliminate spread pricing, and prevent mandatory mail order prescriptions. This bill passed the House unanimously and is expected to be considered by the Senate. Meanwhile North Carolina Senate Bill 479 (SB 479), also known as the SCRIPT Act, was signed into law on July 9, 2025. The ratification of this bill will help make prescription drug costs more transparent by regulating PBM practices.21 Despite differences, both aim to improve transparency and accountability of PBM operations.
Medicaid and Medicare Policy Adjustments
Medicare reforms introduced in 2025 may improve affordability and prescription volume, but concerns remain about the impact of drug price negotiations on small pharmacies.22
Recent changes in North Carolina Medicaid could help stabilize community pharmacy sustainability by increasing covered patient volume. North Carolina Medicaid expansion has added over 600,000 enrollees since December 2023, many (approximately 40%) of whom live in rural counties. This expansion increases the patient base for community pharmacies and introduces fixed per-member payments through managed care organizations, supporting value-based care models.23 In addition, pharmacies are now reimbursed by a fixed payment per enrollee through managed care organizations (MCOs), which increases opportunities for community pharmacies to participate in value-based care initiatives. Both Medicaid and Blue Cross and Blue Shield of North Carolina (BCBSNC) are actively developing ways to reimburse pharmacies for clinical services.
Incentives and Public-Private Partnerships
Targeted financial incentives (preferred provider/“in network” status/enhanced Medicaid reimbursement) may help promote community pharmacy operations in underserved areas. Similar to other programs which have incentivized health care providers serving in underserved areas, considerations may be given to support student loan forgiveness and grants for pharmacists practicing in highest-need areas. Also modeled after existing programs would be the creation of Critical Access Pharmacy Programs. These programs and other options have been explored by public-private partnerships, such as the University of North Carolina at Chape Hill-led Rural Pharmacy Health Initiative. Such programs demonstrate how collaboration between universities, health departments, and pharmacies can improve access in vulnerable communities.
Alternate purchasing models
Community pharmacies can adopt several alternate purchasing strategies to better compete with PBMs and therefore improve their sustainability. Cost-plus pricing models would utilize direct pricing models after evaluating a patient’s co-pay relative to the program’s price. Transparent drug pricing, direct-to-manufacturer purchasing, and partnerships with transparent PBMs are some additional examples. Cooperative purchasing networks or group purchasing organizations (GPOs) may enhance bargaining power, while cash-pay and subscription models attract cost-conscious patients. Finally, value-based contracting aligns pharmacy reimbursement with patient outcomes, opening new revenue opportunities.
Final Thoughts
The closure of North Carolina community pharmacies represents a growing health care crisis, particularly in rural and underserved areas. In addition to providing needed medications, these pharmacies provide essential access points for preventive care, chronic disease management, and public health services. Their closure threatens to widen existing health disparities. Addressing this issue requires immediate, coordinated action. Without swift, multifaceted and coordinated intervention, the continued erosion of community pharmacy infrastructure will have lasting consequences for public health across the state.
Acknowledgments
The author would like to thank Drs. Beth Mills and Penny Shelton for their review of the manuscript.
The author acknowledges the use of Microsoft Copilot™ to assist with editing of the completed manuscript for clarity, grammar, syntax, and length. The author affirms that all opinions, content, data interpretation, and conclusions are his own.
Disclosures
I have no relevant financial conflicts of interest to disclose. I am a member of the North Carolina Association of Pharmacists (mentioned in this article).
{kind=link}