


Background
Access to medications is fundamental to achieving positive health outcomes. Community health centers (CHCs) play a critical role in delivering pharmacy services and comprehensive care to medically underserved populations, often through support from federal programs such as the 340B Drug Pricing Program.
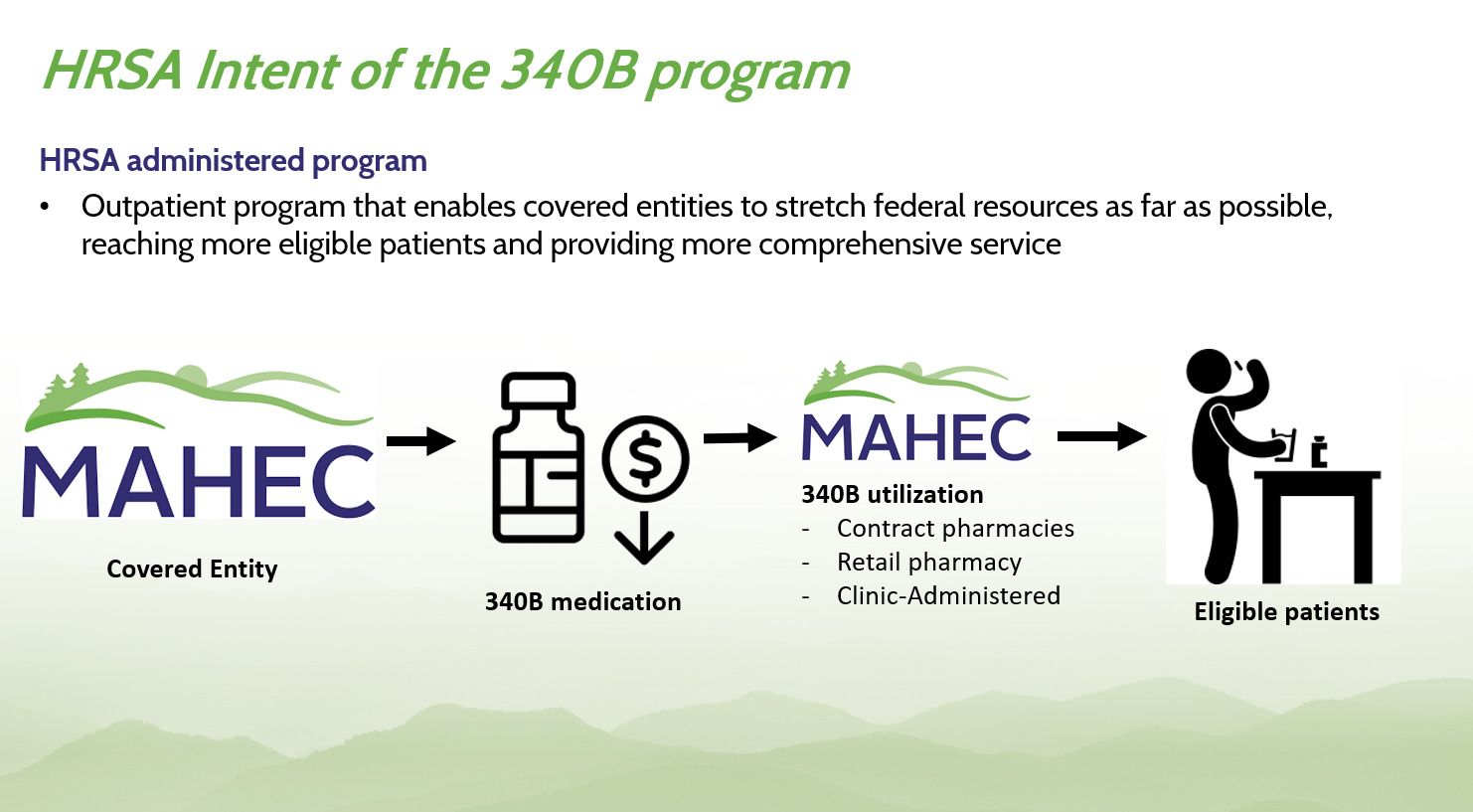
Established in 1992 under the Public Health Service Act, the 340B Program allows eligible health care organizations, known as “covered entities,” to purchase outpatient drugs at significantly reduced prices. These savings enable providers to extend their services, support medication adherence, and improve access to care for patients who might otherwise forgo treatment due to cost or logistical barriers. The program is administered by the Health Resources and Services Administration (HRSA) with oversight from its Office of Pharmacy Affairs (OPA) and is supported by a federally designated Prime Vendor Program.1–3
Pharmaceutical manufacturers that participate in Medicaid are required to offer these discounts to covered entities. In return, covered entities use the savings to enhance patient care, often reinvesting in expanded clinical services, patient education, and pharmacy infrastructure. This partnership is foundational to the program’s success and sustains a safety net for those most in need. A summary of the 340B Program is provided in Table 1 and Figure 1.

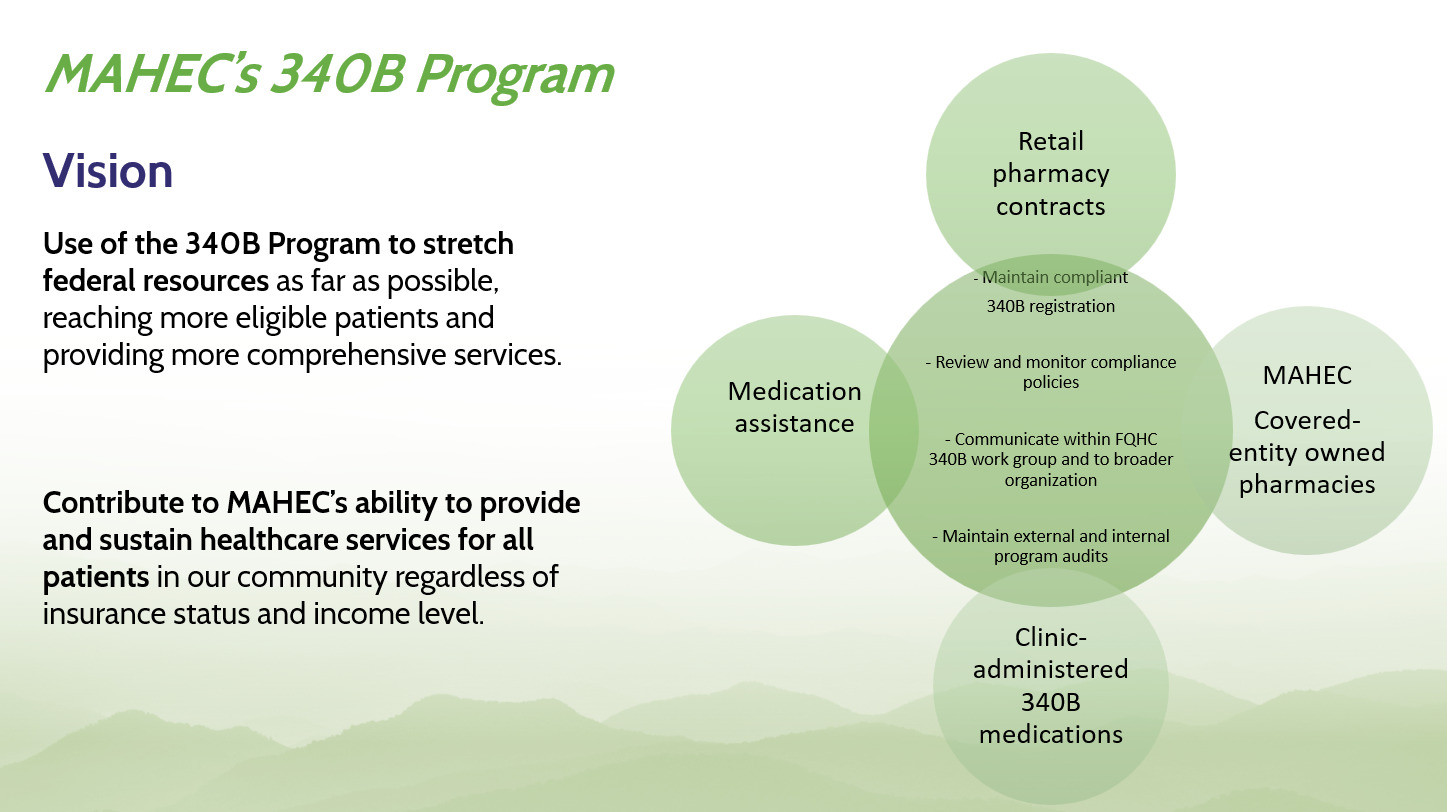
At the Mountain Area Health Education Center (MAHEC), a Federally Qualified Health Center (FQHC) look-alike based in Western North Carolina, the Department of Pharmacy exemplifies how the 340B Program improves local health outcomes (Figure 2 and Figure 3). MAHEC has established on-site pharmacies that allow patients to conveniently fill prescriptions, receive medication counseling, and obtain assistance with navigating complex access issues, including insurance denials, formulary restrictions, and Medicare/Medicaid eligibility. In addition, MAHEC pharmacists collaborate directly with primary care teams across family medicine, internal medicine, and obstetrics/gynecology to support chronic disease management, including diabetes and hypertension.
One example involves MAHEC’s integration of pharmacy services into its maternal health clinics. Pharmacists routinely support pregnant individuals with gestational diabetes, managing medication regimens that are safe during pregnancy while also addressing social determinants that can impact adherence. This kind of team-based approach has been shown to reduce adverse outcomes and improve long-term maternal and infant health.
To further enhance medication access, MAHEC employs pharmacy technicians who specialize in patient navigation. These technicians assist with enrollment in patient assistance programs offered by pharmaceutical manufacturers, charitable distributors, and government agencies. Their work alleviates administrative burdens for patients and providers alike, allowing patients to focus on improving their health.
Consider a common scenario: a patient with multiple chronic conditions, newly insured through Medicaid expansion, is prescribed 5 medications. Without assistance, the complexity of coordinating benefits, navigating prior authorizations, and understanding cost-sharing can overwhelm the patient. At MAHEC, a pharmacy technician works directly with this patient, coordinating with the prescriber and the insurer, locating lower-cost alternatives, and enrolling the patient in a 340B-discounted program—all in a single visit. This intervention ensures continuity of care and increases the likelihood of medication adherence.
A core principle of the 340B Program is that the financial benefit generated from purchasing medications at a discount must be used to expand access and enhance care. This includes providing medications at low or no cost to patients, hiring additional clinical staff, and investing in services that would otherwise be financially unsustainable. At MAHEC, 340B revenues have directly enabled the expansion of pharmacy services and enhanced collaboration across care teams.
Similar models can be found at other 340B-covered entities across the country. For many CHCs, the savings from 340B are used to fund clinical pharmacists who are embedded within medical teams. These pharmacists provide anticoagulation monitoring, HIV pre-exposure prophylaxis (PrEP) services, and substance use disorder (SUD) support. Often, community health centers use their 340B savings to subsidize medications for uninsured patients, ensuring no one leaves the clinic without access to treatment.
Program integrity is essential to maintaining public trust and ensuring that benefits flow appropriately to eligible patients. Covered entities are required to maintain strict compliance with federal guidelines. Drugs purchased under the 340B Program may only be dispensed to eligible patients of the covered entity. Inappropriate use—including diversion to ineligible patients or duplicate discounts—can result in penalties and disqualification. Both HRSA and participating manufacturers play a role in monitoring compliance and safeguarding program objectives.
HRSA conducts routine audits of 340B-covered entities, focusing on the clarity of patient eligibility documentation, drug inventory tracking systems, and separation of 340B and non-340B inventory. At MAHEC, compliance efforts include electronic verification tools, staff training, and internal audits. Pharmacy staff work closely with legal and compliance teams to ensure that all prescriptions processed through the 340B Program meet regulatory standards.
While the 340B Program has faced criticism over the years—primarily centered on whether sufficient oversight exists to ensure patient benefit—its design remains rooted in supporting care for the underserved. Critics argue that the program’s structure allows for variability in how savings are used, and some have proposed changes that would restrict how covered entities use 340B revenue. However, evidence from health centers like MAHEC and others demonstrates that these funds are used responsibly to directly benefit patients.
A 2022 survey conducted by the National Association of Community Health Centers (NACHC) found that 92% of participating CHCs used 340B savings to expand access to medication and services for low-income patients. More than half used the funds to offer services that are not reimbursable under traditional insurance models, such as care coordination and transportation.4
It is important to recognize that while the 340B Program is federally mandated, its benefits are felt at the local level through the relationships between patients and trusted providers at community health centers, children’s hospitals, and public health departments. The strength of the 340B model lies in its ability to channel national policy into community-level impact.
One powerful example of this local impact occurred during the COVID-19 pandemic. Many 340B-covered entities, including MAHEC, rapidly mobilized pharmacy teams to support vaccine distribution, ensure continuity of care for patients with chronic conditions, and deliver medications to quarantined or isolated individuals. The 340B savings helped offset the costs of these emergency responses and ensured that community health centers remained operational despite revenue losses from reduced in-person visits.
Looking forward, the 340B Program continues to be an essential component of the health care safety net. As health systems navigate rising drug prices, staffing shortages, and increasing demand for behavioral health and chronic disease services, the ability to leverage 340B savings becomes even more critical. Policymakers must carefully balance the need for accountability with the program’s original intent, which was to allow covered entities to stretch scarce federal resources as far as possible, reaching more patients and delivering more comprehensive care.
At its core, the 340B Program is about equity. It provides community-based providers the tools to reduce barriers, personalize care, and address the systemic factors that lead to health disparities. While the mechanics of discounted drug pricing may seem complex, the outcomes are simple: more people get the medications they need, when they need them, from providers they trust.
Acknowledgments
The authors have no financial disclosures or conflicts of interest to report.