Building a Framework for Action
The North Carolina State Health Improvement Plan (NC SHIP), launched in 2020, provides a shared framework for advancing the 21 “Healthy North Carolina 2030” (HNC 2030) indicators, which address the social, economic, and environmental drivers of health, also known as “wicked problems”.1
The plan itself represents a static moment in time; however, it is brought to life through 18 cross-sector work groups that comprise the NC SHIP Community Council. Four of these groups were pre-existing statewide collaboratives that were already advancing aligned efforts across the state: the NC Opioid and Prescription Drug Abuse Advisory Committee, the NC State Excessive Alcohol Advisory Committee, the Perinatal Health Equity Collective, and the Comprehensive Suicide Prevention Advisory Council. In 2022, 14 additional work groups were established to foster collective impact on issues for which no formal existing entity was convening in North Carolina. Together, these 18 groups represent the networks and partnerships that bring the NC SHIP to life. The Council convenes representatives from state agencies, health departments, schools, hospitals, community-based organizations, philanthropic partners, and advocacy groups to grapple with issues and actions in real time. Each work group aligns its activities with one or more HNC 2030 indicators, ensuring that local strategies contribute to statewide goals.
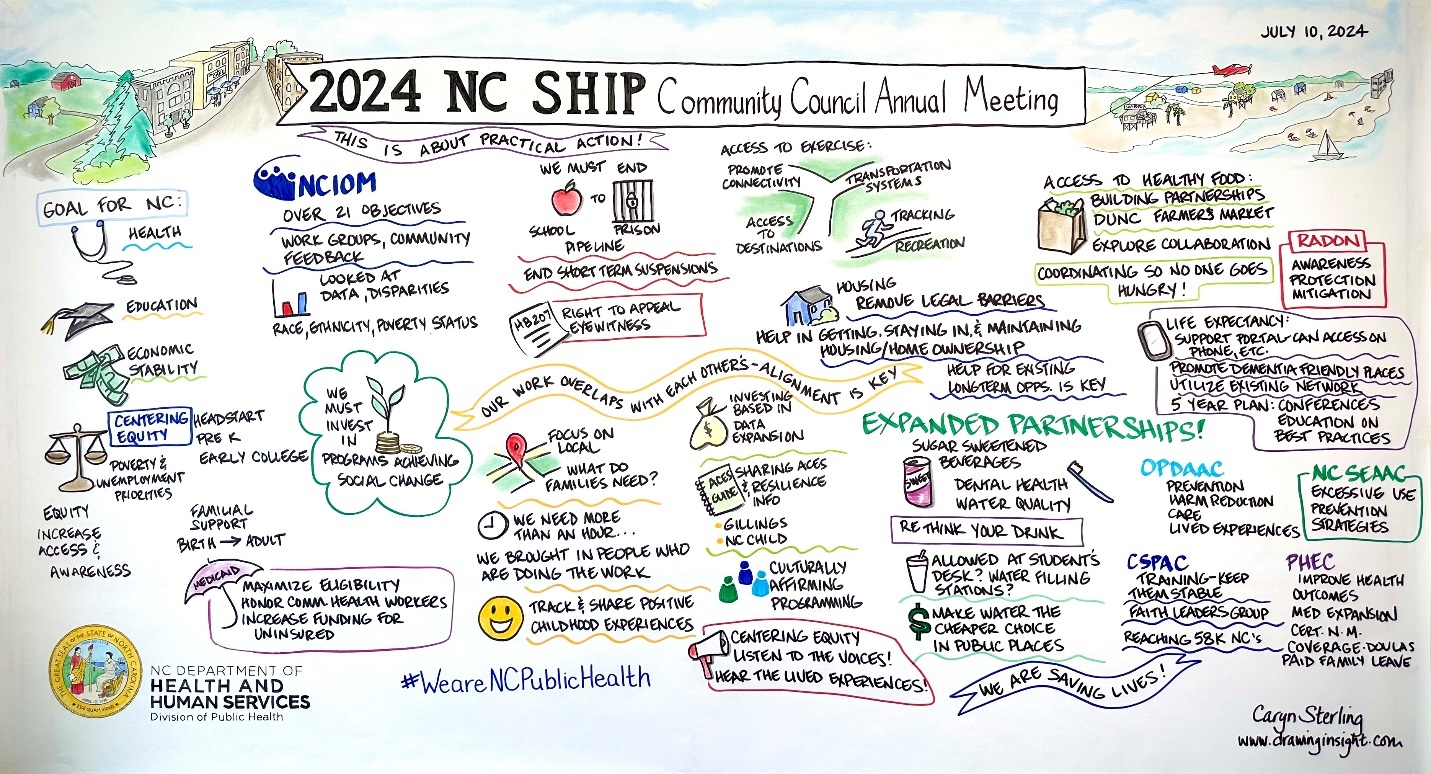
For the newly formed groups, the North Carolina Department of Health and Human Services (NCDHHS) Division of Public Health serves as the convener. Each group is co-led by a trio: someone from state government, a community partner, and a partner organization who all work together to drive the agenda and action of the group. This trio model is innovative and has fostered creativity, shared ownership, and community voice. As the convener, the Division of Public Health is intentional about not being in charge. Groups evolve differently, and that flexibility is part of the design. Key functions of each work group include: 1) coordinating work groups to review data, share strategies, and align resources; 2) integrating NC SHIP priorities with other statewide plans such as the Perinatal Health Strategic Plan and the Strategic Housing Plan; 3) applying Results-Based Accountability (RBA) to track performance and adjust strategies; and 4) hosting an annual Community Council meeting to review progress, spotlight work, and renew commitment (Figure 1).2–4
Successes and Challenges
Collaboration
One of the biggest wins has been the way people work together. The NC SHIP Community Council now brings more than 100 partners to the table each year. That includes health leaders, educators, housing experts, and community advocates. These connections are not just meetings. They have led to joint projects and stronger voices in policy discussions. The Suicide Prevention Advisory Council’s work with rural faith leaders and the Short-Term Suspensions group’s partnership with education advocates are just two examples of collaboration turning into real action. These collaborations are often catalysts—moments of connection that ignite projects or strengthen networks. Even when they do not lead to formal initiatives, the trust and relationships formed are valuable outcomes that strengthen the state’s public health system.
Data-Driven Decision Making
Another strength has been the use of data to guide decisions. HNC 2030 indicators and local dashboards give work groups a clearer picture of where progress is happening and where gaps remain. When overdose deaths spiked, opioid data helped shape prevention strategies and expand naloxone distribution. Perinatal health data has also been key to advancing doula reimbursement and safe sleep efforts.
Community Voice
NC SHIP partners have shown the importance of listening to communities and tailoring approaches. The ACEs (Adverse Childhood Experiences) Work Group has worked to lift up culturally rooted supports, while the Sugar-Sweetened Beverage Consumption Work Group used local television and SNAP-Ed to encourage families to choose water. These are not one-size-fits-all campaigns. They are built to meet people where they are. The Life Expectancy Work Group also built on community input by developing outreach and training materials that link fall prevention and brain health. They highlighted the connection between dementia care, chronic disease risk, and safe home environments, and even partnered to promote radon education materials translated into multiple languages.5
Policy Impact
Finally, there has been influence at the state level. From paid leave and childcare access in perinatal health to the Department of Health and Human Services’ (NCDHHS) 5-year Strategic Housing Plan, work group recommendations are shaping how North Carolina addresses the root causes of health.

Challenges
Engagement. One ongoing challenge is keeping people involved over time. Turnover among leaders and members means groups sometimes lose momentum, even with better onboarding processes in place.
Data access. Another barrier is timely, detailed data. County-level or population-specific information can be slow to arrive, which makes it harder for groups to shift strategies quickly. Alcohol prevention work was delayed in part because federal staffing shortages slowed updates.
Alignment. Coordinating across statewide plans is also difficult. With efforts like the Early Childhood Action Plan, All Ages, All Stages NC, and NC Strategic Housing Plan all moving forward, it is not always easy to avoid duplication. Partners are committed, but the landscape is crowded. This challenge is compounded by a changing landscape of funding priorities and shifting state initiatives, which requires partners to continually adapt.
Measuring Impact and Community Benefit
Strengthened collaboration. Partners report that working through NC SHIP has helped strengthen relationships and create new ways to coordinate efforts. Suicide prevention work with rural faith leaders, perinatal health partnerships with childcare and maternal health advocates, and housing initiatives that link health and stability are examples of this collaboration in practice.3
Policy and systems change. Collective advocacy has influenced Medicaid expansion rollout, expanded food security programs like Double-Up Food Bucks, and supported housing and perinatal health priorities.2,3
Capacity building. Partners report that skills in results-based accountability and equity-centered planning have enhanced their ability to apply for grants, measure outcomes, and demonstrate impact to funders.6
Scorecards. Progress is tracked publicly through the Healthy North Carolina 2030 Scorecard and the NC SHIP Community Council Scorecard. These tools allow both partners and the public to monitor trends, compare progress to targets, and identify areas needing attention.3,4,7
Feedback. Annual surveys and meeting evaluations capture lived experience and community perspectives, helping guide course corrections.
Alignment. Each work group maps its strategies to HNC 2030 indicators, providing accountability and transparency for the work.
Conclusion
At the halfway point of Healthy North Carolina 2030, the NC SHIP Community Council demonstrates the value of collective impact in addressing complex health challenges. Successes include new collaborations across sectors, data-driven strategies, community-rooted approaches, and policy influence in areas such as perinatal health, housing, and education.
Challenges remain in sustaining engagement, securing timely data, and coordinating across statewide plans. These challenges reflect not only the crowded space of state initiatives but also shifting funding landscapes that require continual pivots.
Over time, NC SHIP has shifted from convening new groups to supporting existing efforts where leadership already exists, moving from convener to supporter. These pivots illustrate the importance of community ownership and adaptability, which are features critical to sustaining progress in a dynamic health environment. The NC SHIP Community Council’s work shows that North Carolina communities benefit when diverse partners align their strengths toward shared goals, building momentum for a healthier state.
Acknowledgments
The author thanks the NC SHIP Community Council members, co-leaders, and partners for their dedication to improving health in North Carolina.
Declaration of interests
The author has no conflicts of interest to declare.
Financial support
The author has no financial support to report.
Corresponding author
Address correspondence to Ashley Rink, North Carolina Department of Health and Human Services, Division of Public Health, 1915 Health Services Way, Raleigh, NC 27607 (ashley.rink@dhhs.nc.gov).