Introduction
Intellectual and developmental disabilities (IDD) are a group of conditions characterized by impairment in physical, intellectual, or emotional development. These conditions typically present early in an individual’s life, but can also appear later, and persist throughout their lifetime.1 Examples of IDD include autism spectrum disorder, intellectual disability, cerebral palsy, and other developmental delays.1 The United States’ prevalence of IDD is estimated at 8.56%.2 Many individuals with IDD have decreased communication ability, increased sensitivity to sensory stimuli, experience challenges with new environments, and rely on familiarity.1,3–5 These factors significantly impact their daily functioning in addition to their ability to obtain dental care.4
Compared to individuals without disabilities, those with IDD are more likely to face barriers to dental care and experience delays in necessary dental treatment.6,7 This begins in childhood and significantly increases in adulthood. This is, in part, due to few generalist providers accepting individuals with IDD.7 Additionally, the transition to adulthood for individuals with IDD is typically accompanied by reliance on Medicaid and other public insurance options.8,9 North Carolina adult Medicaid benefits are quite comprehensive, including no spending limits and coverage for most preventative measures.10 This has not translated into increased acceptance among providers, with North Carolina ranking 37th out of 50 states in Medicaid acceptance.11
Lack of dental care and unmet dental needs can cause dental pain and infection and have been linked to systemic diseases.12 While many pediatric dentists continue to care for individuals with IDD into adulthood, treatment needs often progress past the scope of pediatric dental care. An adult and aging population requires services not typically performed by pediatric dentists (e.g., dentures, root canals, implants, and other procedures). Thus, identifying and decreasing barriers is important for establishing a long-term dental home.13 The ideal dental home would provide a place for comprehensive and consistent dental care for an adult individual.14
The size of this population in North Carolina, estimated at more than 230,000 people, and the lack of providers that care for them create the need to better understand barriers of care, particularly at the point of care transition.15 While some evidence regarding dental care transition exists, little qualitative research has been undertaken on the topic. This study utilized interview data across multiple groups to identify and better understand perceived barriers to dental care transition for this population.
Methods
This study entailed recruitment and one-on-one interviews with different groups. These groups included families of individuals with IDD, pediatric and general dentists, and access-to-care experts. The study received ethics approval from the University of North Carolina at Chapel Hill Institutional Review Board (22-0962).
Recruitment
Recruitment of family caregivers (n = 19) was accomplished through partnerships with Simons Foundation Powering Autism Research (SPARK) and North Carolina family support groups. SPARK, one of the largest autism research organizations, and family support groups were identified due to their large base of available families for research within North Carolina. Multiple meetings were held with each organization to establish goals and parameters before subject recruitment. Partnering organizations aided recruitment by facilitating email and social media postings. All partnering organizations did not receive direct benefits, besides contributing to knowledge of this topic.
Eligible participants met the following criteria:
-
Must reside in the state of North Carolina.
-
Must have an individual in their immediate family (son, daughter, or other immediate relative) with IDD of at least 18 years of age.
-
Must have at least attempted dental care transition between a pediatric and a generalist provider at some point in the individual’s life.
Exclusion criteria included no access to either cell phone or laptop for communication. One interview was granted per family, even for those with multiple individuals with IDD. Agreeing families were offered compensation ($35 gift cards) for their participation, with some declining for various reasons. Participation was offered to Spanish speaking individuals, but none consented. Characteristics about the participants are described in Table 1.
Recruitment of pediatric dentists (n = 5) and general dentists (n = 4) was done via an email invitation sent to the North Carolina Dental Society, an organization with over 3900 members. An initial email was sent; a follow-up one was sent 30 days later. The inclusion criteria were an active license and practicing in the state of North Carolina, while all investigators and full-time dental school faculty were excluded. All provider participants were selected due to their knowledge regarding the topic and experience with dental care transition for IDD populations.
Lastly, email contact was made to North Carolina Medicaid representatives and Project Accessible Oral Health, a national organization involved in improving health equity for those with disabilities. All (n = 3) were open to discussion points and were chosen due to their ability to comment on broader aspects not mentioned by other participants.
Recruitment and interviews continued until conceptual depth was achieved and no new themes emerged. Conceptual depth was chosen as the metric due to its well-established and understood definition and criteria.16 Interview and data analyses were performed by the same investigator. The decision to interview 3 separate groups was made to achieve data triangulation and find commonalities of themes among those with different perspectives.
Data Collection
Semi-structured interviews lasting between 30 and 60 minutes were conducted via phone and video-conferencing software (i.e., Zoom and WebEx) by the principal investigator at times convenient to participants. Customized questionnaires for each group were made (Appendices A, B, and C). Written and verbal consent was obtained from all participants. Interviews were recorded and then transcribed verbatim using transcription services (Rev software). De-identification of transcripts was done for confidentiality.
Data Analysis
Transcribed interview transcripts were imported to qualitative research software (MAXQDA 2022). A conventional content analysis was used as the qualitative methodology; it was chosen due to its widely accepted use and understanding.17,18 Unlike some other qualitative methods, traditional content analysis does not rely on predefined codebooks or references.17,18 As a result, data is more likely to be free of bias or preconceived notions.17,18
Coding was done by the principal investigator, consisting of reviewing transcripts and identifying commonalities among each participant group. Two investigators, also dentists with experience in transition of care, served as auditors and re-read transcripts to validate coding, a practice often used by qualitative researchers.19 Disagreements regarding coding were few, but the research team would meet to establish consensus. Conceptually similar codes were grouped together to create comprehensive themes (Figure 1).
Coding was done under the guidance of a senior qualitative researcher. The senior qualitative researcher met regularly with the principal investigator to discuss coding, codebook evolution, codes and findings. As a co-author, he also provided recommendations on identifying and naming themes.
Results
Participants were forthcoming with their experiences and perspectives on the topic. The most prevalent themes for each group are discussed below and are summarized in Table 2, alongside additional illustrative quotes.
Family Themes
Perceived lack of experience from providers. All families agreed that finding a generalist provider comfortable with treating individuals with IDD is a prominent barrier during transition. Most families (83%) reported calling several offices without success. Even when an office would accept them, interviewees reported a general lack of experience and comfort of many generalists in treating individuals with IDD. This often led to dissatisfaction in level of care and short duration of stays at an office.
“Well, the first and foremost is, there’s just not many people who do it, who say they do it. And I don’t mean this in a bad way, but I just get the feeling that nobody has any training to deal with people with [IDD]” – Family 5
Even families residing in urban areas of the state struggled when searching for a generalist provider; these families reported that offices would be accepting new patients but were not receptive to seeing individuals with IDD. Often, the denial occurred before attempting to see the individual.
“We called five [offices]. Even a new dentist facility, new doctor. And they were saying, ‘We accept new patients.’ We call, we make an appointment, we say that we have Medicaid. ‘Oh yes, we’ll take.’ And then after [identifying patient has autism], say, ‘Oh no, we don’t.’ I’m like, ‘We did it. You say new patient, I mean, which kind of new patient [do] you take?’” – Family 8
Long waitlists and far distances hinder care. For families that were able to find providers with comfort treating individuals with IDD in their area, additional barriers, including long waitlists and inadequate staffing, impeded timely care.
“The first consultation…I want to say it was at least a quarter of a year if not more, to get in for that… [the next appointment] it was probably pretty close to a year if not more.” – Family 7
Many families (50%) were willing to leave their area and travel further distances to find a willing provider. For some, however, they could not justify traveling far distances to seek dental care for their family members.
“So, the thing is, is that if there were other options I may have discounted them altogether based upon how far away they were [from us].” – Family 7
Frustrations from insurmountable barriers. For some (28%), the numerous barriers faced when attempting transition led to forgoing dental care. Although all participants expressed the importance of dental care, the many barriers were too much to overcome for some. These participants stated their family members had not received dental care in a significant amount of time, in some cases 10 years, due to these barriers.
“We are in complete limbo-land along with I know a ton of other people in our community. All of us are in the same boat, where we’ve aged out of the pediatric dentist world and there’s nobody to take the place.” – Family 11
Some families reported that their family member required many health care services, and they had limited time. The lack of time and bandwidth has led to de-prioritization of oral health care for them.
“So, we’re dealing with speech, we’re dealing with OT, we’re dealing with PT, we’re dealing with behavioral therapists, we’re dealing with what’s happening in the classroom, we’re trying not to get punched in the face. We can’t find a dentist. We’re like, ‘Oh, well.’” – Family 2
Lastly, many families are referred to dental schools but often have trouble receiving appointments, getting off waitlists, and reaching staff for appointments.
“You call; they’re not taking patients. ‘No, we don’t do that.’ And it’s like, ‘Really?’ And so, someone suggested actually [the dental school]. So that’s been the most recent thing, but I can’t get anyone to call me back.” – Family 9
Dental Provider Themes
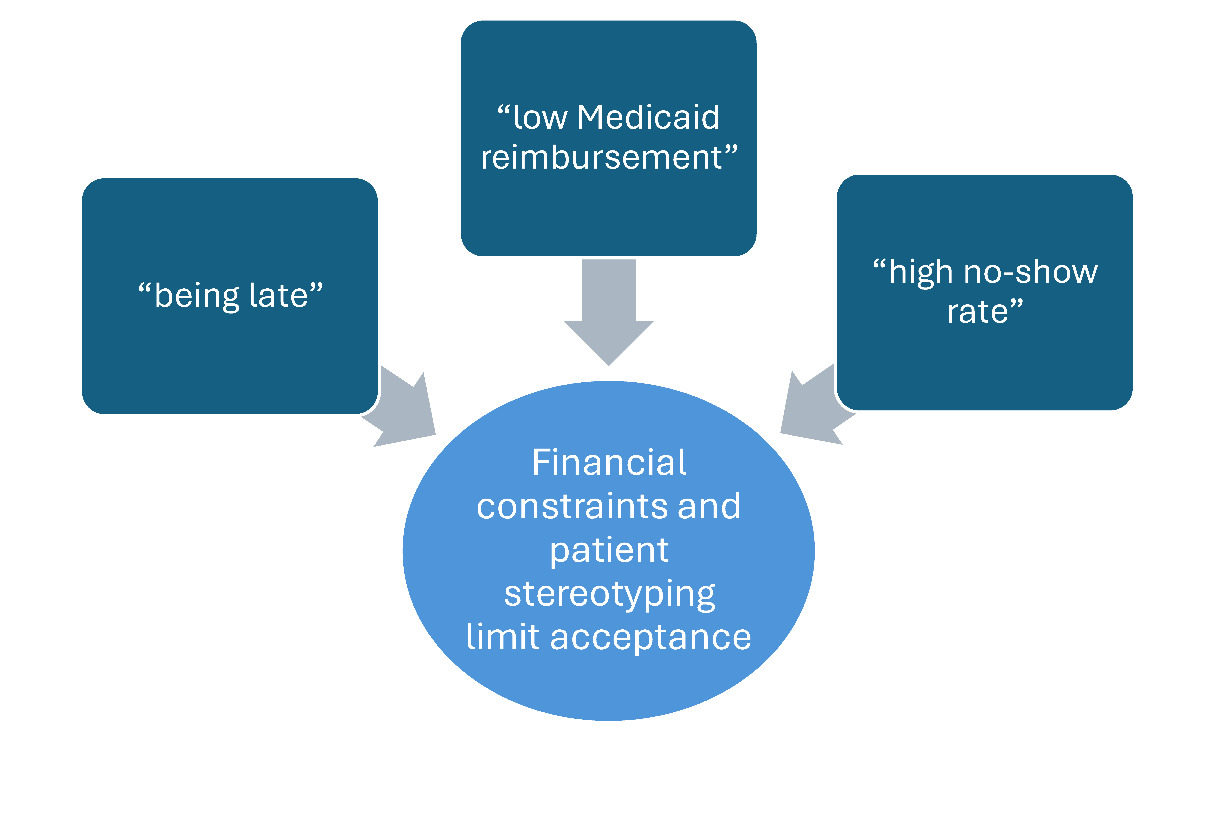
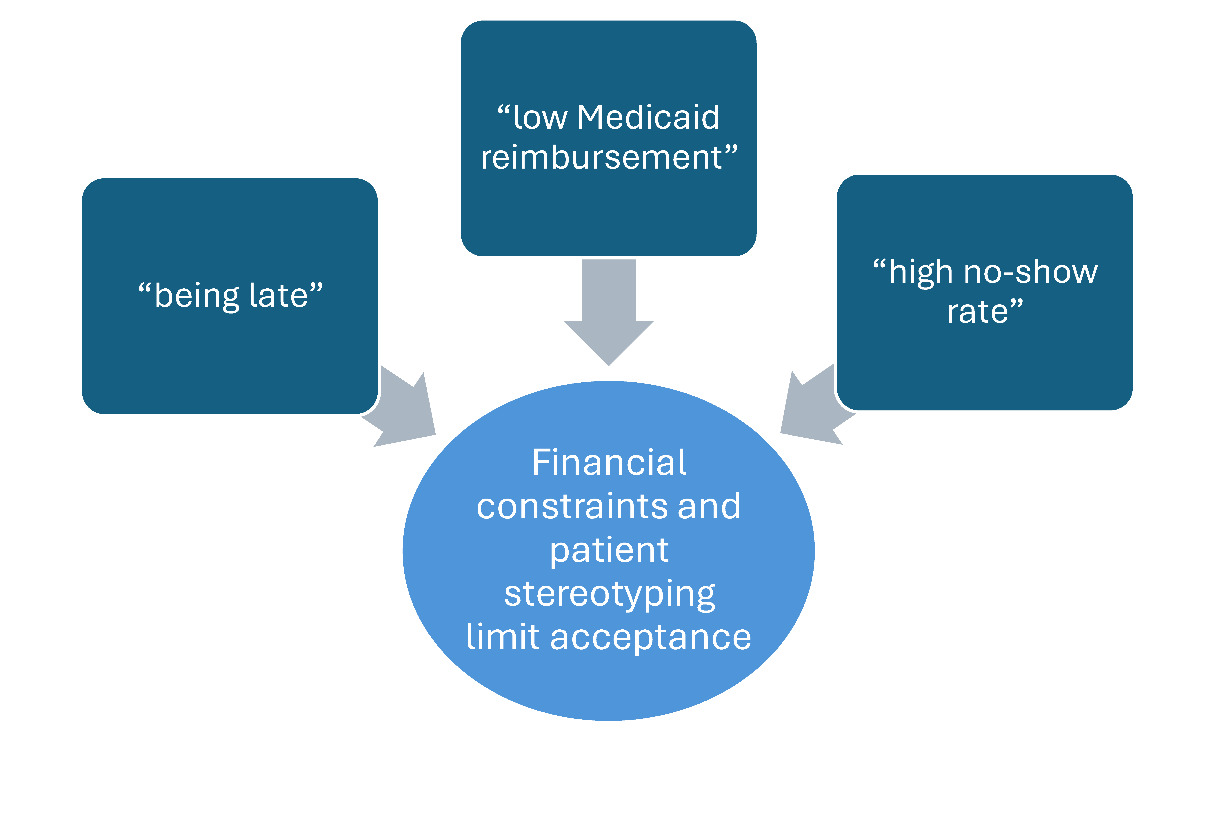
Financial constraints and stereotyping limit acceptance. Most individuals with IDD qualify for Medicaid in North Carolina, but many providers do not accept it.8,9,20 Those not accepting Medicaid cite concerns regarding low reimbursement rates, among other detractors. For those open to treating individuals with IDD, this is a prominent reason for not accepting IDD populations into their practice.
“So, the cost of rendering care to those patients is a barrier. Even if the dentist knows how to handle and work with patients who have special health care needs, they may not do it, because they don’t think they’re reimbursed at the [proper] level.” – Provider 1
Providers often spend considerable additional time caring for individuals with IDD without corresponding reimbursement. Often, individuals with IDD require significantly more time to receive dental treatment.21 Dental reimbursement is given for a specific procedure, irrespective of the amount of time it takes. This limits the number of patients able to be seen, further deterring providers from accepting this population.
“Because Medicaid doesn’t cover what it should as far as that extra time…we’re really donating our care to these folks and not making money. We lose money every time we see these patients.” – Provider 9
Many providers (67%) also discussed frustrations with the additional costs of maintaining Medicaid systems and cumbersome administrative processes.
“The other thing is just the hoops you have to jump through with Medicaid and the pre-authorizations with Medicaid…so people just throw up their hands and don’t do it.” – Provider 6
Lastly, stereotypes of Medicaid populations, such as higher no-show rates and low compliance with care, are pervasive and impact providers’ willingness to accept public insurance (56%). Because individuals with IDD most often qualify for Medicaid, widespread stereotypes are often cast on this population and affect their ability to be seen.
“There’s a whole, overall systemic issue that these patients historically break appointments more and need more operative work. And so, I can’t give up more block time for patients who either are not going to show or who I’m going to get paid so little to see.” – Provider 7
Lack of staffing, proper equipment, and interruptions to clinic flow. Irrespective of reimbursement, many offices (56%) struggle with the incorporation of IDD populations into their practice. Providers express concerns about how and when individuals with IDD can be seen efficiently, especially for offices focused on operative care.
“In a busy general practice where they’re trying to do restorative [work] including implants and just keeping up a normal hygiene schedule, it’s hard for them to incorporate someone who might not tolerate normal treatment very well.” – Provider 5
Providers discussed how allocating staffing (33%) for treatment of IDD populations can be difficult, especially amidst pervasive staffing shortages.
“You need to have your staff know how to deal with [IDD populations] …it’s tough with staff almost wanting double [pay] from pre-COVID.” – Provider 2
Others (33%) cite fear of how mixing individuals with IDD with other groups could affect patient satisfaction. Practices were especially worried about how waiting rooms and open-bay settings could be managed when treating individuals with and without IDD simultaneously.
“When you think about the idea that you may have a person with autism in a waiting room and they may be rearranging the furniture, or they may be acting different and they’re mixing with patients that may not understand that, it affects the whole practice.” – Provider 1
Finally, many practices (44%) cite the lack of proper equipment necessary (e.g., protective stabilization and sensory equipment) for the treatment of some individuals with IDD. Offices that do not typically care for IDD populations are often not properly equipped to do so.
“We have a [stabilization] board for some of them, because otherwise it just won’t be safe for us to work on them…that could be an issue with general dentists, too. They’re not used to using that type of equipment that we use.” – Provider 3
Larger Access to Care Themes
Poor workforce preparedness. Though enhancements in dental school curricula have been made in this area, a widespread lack of comfort remains. The current Commission on Dental Accreditation (CODA) states that dental students “must be competent in assessment of patients with special needs,” with no specific requirements.22 Experts agree that current standards of care are vague and fall short.
“We have not, in dentistry, in [the state] and I think nationally, developed a way to educate general dentists that’s more comprehensive other than voluntary CE courses, elective CE courses they might take. And that is kind of sad.” – Access Expert 1
“Providers need a lot of education and training related to how to serve …. this special population. And I think I would love to see something like that truly, truly ingrained in curricula really across the country and not just a one class session.” – Access Expert 3
Additionally, access to care experts believe that delivering care to individuals with IDD is not drastically different from treatment of other populations. Better education and experiential training should lead to improved confidence and provider comfort.
“I think they are [equipped] just based on the knowledge that they already have about dentistry, but I don’t think they have the confidence to do it. To me, treating a person with a developmental disability is not all that different than treating someone without one.” – Access Expert 2
Offices using discriminatory practices for patient acceptance. Access to care experts acknowledge that many practices exhibit discriminatory practices when screening patients, with many offices declining care or referring them before even seeing the patient. State and national level dental agencies strive to address this issue, but it is still prevalent.
“I know that it happens, I’m not happy. I know that sometimes they’ll say, ‘Along the autism spectrum, we’ll see these patients, but we won’t see these patients’… I have heard of cases where the staff are giving out information that the provider really doesn’t want them to say to patients, because for one reason or another, [the office] doesn’t want that group of patients treated in the practice.” – Access Expert 1
Experts also believe that these practices are troubling given that many individuals with IDD can be treated in dental practices without advanced interventions.
“Yes, of course there’s going to be that 5%, where the most extreme behaviors [or] the most medically complex…but to turn away that 95%, just because of the assumption of the diagnosis, is absolutely ridiculous. And there’s so many little things, tweaks and tools, and things like that that can be easily implemented in a practice, and not expensive, but simple.” – Access Expert 2
Discussion
Many common themes and similarities were seen across all participant groups. All agreed that an unacceptably small number of generalist providers are seeing individuals with IDD within the state. There are several reasons for this, including a general lack of comfort among providers and poor reimbursement rates for care, particularly from Medicaid. Sub-optimal didactic and clinical education within our current dental school curricula most often resulted in a lack of provider comfort. Lack of reimbursement is particularly troubling for providers given that many individuals with IDD require increased time for care.23
Regarding lack of experience, a concerning finding is the lack of provider attempts to see individuals with IDD before referring. Participants agree that this is, in part, due to inadequate education and reimbursement levels, but it is also tied to a current lack of willingness to attempt care for this population. Autism and other IDD diagnoses are spectrum conditions that have a wide degree of variability, many of whom do not require advanced behavioral management.24 Without willing generalist providers, patients either stay with a pediatric provider, are referred to a dental school, or go without care. The American Academy of Pediatric Dentistry (AAPD) offers guidance regarding transition, including the suggestion to stay with an individual’s pediatric dentist in the interim during transition.14 Staying with a pediatric provider indefinitely, however, raises ethical concerns, as adult and aging patients require procedures not within the scope of most pediatric dentists.
There is a general lack of Medicaid acceptance within North Carolina, irrespective of IDD population. In 2023, only 35% of dentists participated in Medicaid within the state, leaving many counties without any Medicaid providers.11 Additionally, dental Medicaid reimbursement rates have not significantly changed in 15 years.25 This further limits provider options, as most individuals with special health care needs use Medicaid.8,9 While inclusion of IDD in state Medicaid eligibility is well-intentioned, it is currently a model that increases vulnerability of an already susceptible population. Those with IDD are found to be at increased risk for poor oral health, and the state’s current Medicaid climate leaves them without many viable options.26
All the barriers in our current system increase the pressure on already-inundated dental school and specialty clinics as safety nets for this population. Families and access to care experts highlighted the lengthy waitlist, often over a year, to obtain consultation; another wait occurs before any treatment is rendered. This lag impacts the quality of oral health care and may contribute to urgent dental needs (e.g., pain and infection) for this population.
There was some overlap between the themes of this study and those previously identified in literature. The previous studies were done many years ago, showing lack of meaningful improvement in known barriers on the state and national level.27–29 In addition to the already-known themes, it appears the geographic distribution of providers within the state provides significant hinderance to families. With only 3 dental schools and few accepting private providers, many families give up and cease to seek care, exacerbating oral and dental problems.
While barriers to care were the focus during conversations, multiple families discussed the success of having a generalist provider within their existing pediatric practice. A hallmark of many IDD conditions, particularly autism, is the need for familiarity and repetition.5 Although the provider was changing, the rest of the office was unaltered (i.e., dental assistants, hygienists, and other support staff). This model of care can provide transition without significant gaps of coverage and maintain patient comfort. This could be a promising avenue to aid transition, especially in areas with the most need.
Limitations
All IDD conditions may not be represented in this study. Another perceived limitation is older individuals being included in this study. This may give the appearance of outdated circumstances and barriers for those who attempted transition many years ago; however, literature shows that barriers have changed little over time.30,31 Caregivers conducted interviews, mainly due to the severity of the individual with IDD’s condition, which may not fully represent the affected individual’s feelings. Other limitations are the sample sizes of the providers and access-to-care experts. The sentiments, however, were largely very similar across all interviews, demonstrating a likely translation to a larger population.
Conclusion
The study identified many notable barriers for dental care transition for individuals with IDD, the most prominent being the lack of providers, sub-optimal provider education and experience, and low Medicaid acceptance and reimbursement rates. Discriminatory practices for accepting patients appear to be highly prevalent. Recommendations for improvement include higher Medicaid reimbursement rates and improved education for providers. Regardless of any new care models, all participants agreed that increased general dentist participation is necessary to achieve optimal oral health care for this vulnerable population.
Acknowledgments
The authors would like to acknowledge the support of Simon Foundation Powering Autism Research (SPARK) and all other parties for their efforts in recruitment.
Financial support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Disclosure of interests
The authors have no conflicts of interest to declare.