Introduction
Sir William Osler, the Father of Modern Medicine, said, “He who knows syphilis knows medicine.” Congenital syphilis rates in the United States have increased 700% in the past decade.1 The Southeastern region of the United States, home to 8 of 10 non-Medicaid expansion states, has experienced a 206% increase in syphilis rates during the same period.2,3 While men account for most reported cases of syphilis, the rate of increase in women is exceeding that of men.3,4 The increase in female syphilis infections is associated with a 755% increase in congenital syphilis (CS) between 2012 and 2021.5,6 The impact of CS in newborns is profound, ranging from asymptomatic or mild symptoms that resolve with treatment to devastating clinical sequelae, stillbirth, and neonatal death.7
Syphilis is detectable and treatable, therefore congenital syphilis (CS) is entirely preventable. Most states have laws requiring syphilis testing during pregnancy, but they vary across jurisdictions, just as guidance from the national medical and public health community does. The lack of alignment on recommendations for syphilis screening in pregnancy issued by major professional organizations, public health agencies, and individual state mandates exacerbates an already complex issue. While there appears to be general agreement on the benefit of a first-prenatal-care-visit syphilis screening, the recommendation for additional screenings usually depends on the provider’s assessment of patient risk or residence in a high morbidity jurisdiction. Additionally, oftentimes state laws mandating syphilis screening during pregnancy differ from professional organization recommendations.8,9 The inconsistencies in practice as well as the emphasis on individual provider assessments leave room for bias and missed diagnoses.
Timely diagnosis and treatment are essential to prevent avoidable complications of CS. Antibiotic treatment is highly effective when provided early in the infection. The recommended treatment is penicillin G benzathine (Bicillin), which is currently in short supply in the United States and the only recommended course during pregnancy.10 If an infected individual has a penicillin allergy, they must be desensitized and treated. Appropriate and timely treatment can prevent CS in about 98% of cases.11
Nationwide, CS rates rose 755% between 2012–2021.5,6 The Southeastern United States has been impacted more than other US regions, and rates of syphilis in women and babies continue to outpace other regions. While the states in the South make up less than one third of those in the country, they account for over one half of the cases of CS. The Southeastern United States has unique challenges when compared to other regions. Only 3 of the 11 Southeastern US states in the partnership had implemented Medicaid expansion at the time of this intervention.12 This leads to a greater number of individuals who lack health insurance, which is a barrier to accessing health care, including preconception care. The 11 Southeastern US states together average about 10% of the population without health insurance, compared to the national average of 8%. It is important to note that the Southeastern states with expanded Medicaid at the time of the intervention have an uninsured percentage below the national average.13
The demographic composition of the Southeastern United States may also be a contributor to the region’s disproportionate rates of CS. Over half of the US Black population resides in the South.14 There is also a significant Hispanic/Latino population in several Southeast states, including Florida and Texas.15 Higher rates of maternal syphilis and CS are seen in Black, Hispanic, and Native American communities due to systemic barriers, such as limited health care access, economic opportunities, transportation, and education. Even with testing, inadequate treatment in Black/African American and Hispanic/Latino communities is the most common missed opportunity to prevent CS in those communities.6
Medicaid covers approximately half of pregnancies and newborns in the 11 Southeast states engaged in the partnership described in this paper.16 Consistently, across all the states that have conducted a cost analysis, the total cost of care for a baby with CS is higher than that of an uninfected newborn, and the increased costs persist in the first 5 years of life. These costs exclude the physical and psychological impact on the lives of affected birthing people, newborns, and their families.
To drive health equity, obtain a better understanding of the challenges facing Southeast states, and identify actionable solutions to rapidly address the rising incidence rates of CS, public health and public payer leaders from across the Southeast convened to identify and implement interventions. This study analyzes and summarizes the outcome of a necessary yet uncommon collaboration between public health and public payers from multiple states, facilitated by leaders from the North Carolina Department of Health and Human Services.
Methods
The approach to the initiative was multifaceted, involving pre-summit sessions, the in-person summit, and post-summit convenings. Initially, commercial and public payers from the Southeastern United States were identified, with a focus on Medicaid leaders and Medicaid Managed Care Organizations. Simultaneously, Department of Public Health leaders for each state were also identified and invited to participate. Centers for Medicare & Medicaid Services (CMS) and Centers for Disease Control and Prevention (CDC)/CDC Foundation representatives were invited to participate as well. These leaders had various backgrounds, including public health professionals and clinicians whose backgrounds spanned multiple specialties, including obstetrics and gynecology, pediatrics, family medicine, infectious diseases, and emergency medicine. The three pre-summit sessions were designed to engage perspectives from “the person”, “public health”, and “the payer.” The pre-summit sessions were opened to any interested party, and recordings of the sessions were made available for those unable to attend in real time. The in-person event limited participation from each state to ensure the size of the gathering was large enough for state representation, yet nimble enough for rapid action.
The first webinar, “Remembering Our History with Congenital Syphilis and the US Public Health Service Study on Syphilis at Tuskegee,” set the stage for future discussions by acknowledging the history of abuse and stigma of syphilis in the United States. The second webinar, “Congenital Syphilis Surveillance and Clinical Case Definitions,” provided an opportunity for participants to get updated information on the current state of congenital syphilis in the Southeast and establish an understanding of case definitions. In the last pre-summit webinar, “Payer Perspective on Congenital Syphilis Landscape,” participants learned more from state Medicaid agencies. The in-person summit was a one-day interactive and strategic planning event. Participants left the meeting with action items to take back to their respective jurisdictions. The post-summit virtual convenings provided an opportunity for updates, action item review, and discussion of next steps.
Results
An analysis of variation across state public health statutes on syphilis testing in pregnancy was discussed at the summit. Additionally, the actual rates of CS were shown, revealing that there was little concordance between public health statutes and outcomes (Table 1).8,17
A comparison of recommendations across major provider associations and national organizations was reviewed at the time of the summit and revealed ambiguity as well as variation.18–21 The American Academy of Pediatrics (AAP), American College of Obstetricians and Gynecologists (ACOG), and Centers for Disease Control and Prevention (CDC) prenatal syphilis screening recommendations were aligned. American Academy of Family Physician (AAFP) prenatal syphilis screening recommendations supported that of the United States Preventive Service Task Force (USPSTF), which did not include a 3rd trimester screen. At the time of the summit, ACOG, AAP, and CDC guidelines recommended 3rd trimester and delivery.
After reviewing public health statutes and the evidence-based guidelines, summit participants voted on the most appropriate guidance given the current rates of CS in the Southeast (Figure 1). Participants aligned on testing at the first pregnancy visit, between 28–32 weeks gestation, and at delivery. Of note, a robust discussion on what “first visit” means revealed that many practices wait for prenatal labs until the first formal intake pregnancy visit, which can be delayed into the late first trimester or early second trimester. To this point, obtaining the syphilis test at the first prenatal encounter rather than the first formal prenatal visit is critical to avoid delayed diagnosis in early pregnancy. Additionally, attendees agreed on the best practice of documenting the birthing parent’s syphilis results on the hospital chart prior to discharging the baby.
The Group Think session on payer levers to reduce the incidence of CS resulted in dozens of recommendations that fell into 5 major categories:
-
Tracking and reimbursement to support universal guidelines to test pregnant women at the first pregnancy visit, 28–32 weeks gestation, and at delivery.
-
Communication across all payers to align on the above standard.
-
Launching a social media campaign to raise awareness among the public and providers.
-
Development of value-based incentives to motivate providers to test at the desired intervals.
-
Mobilizing care management and/or home visits for all pregnant persons not meeting testing guidelines or with a positive syphilis test in pregnancy.
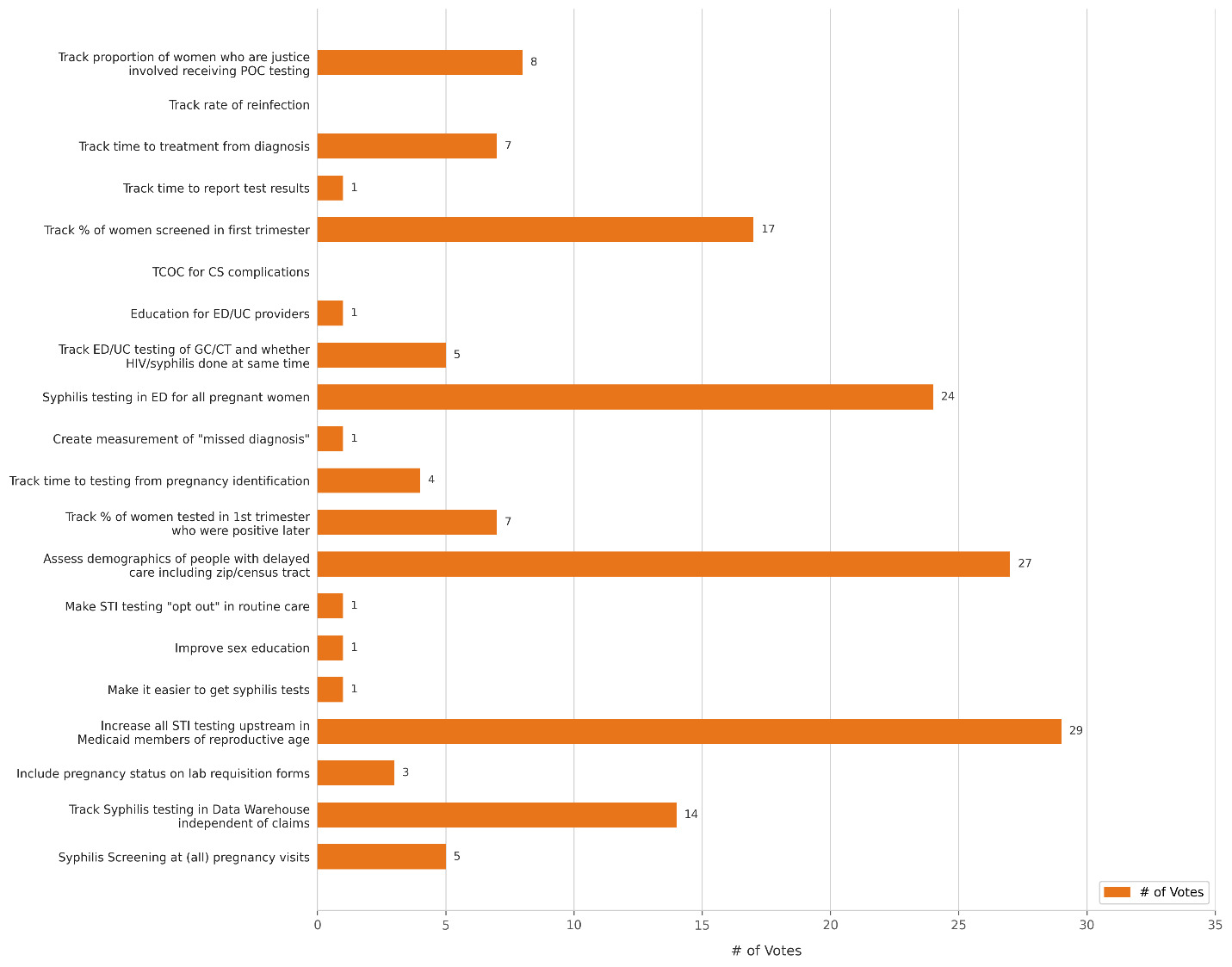
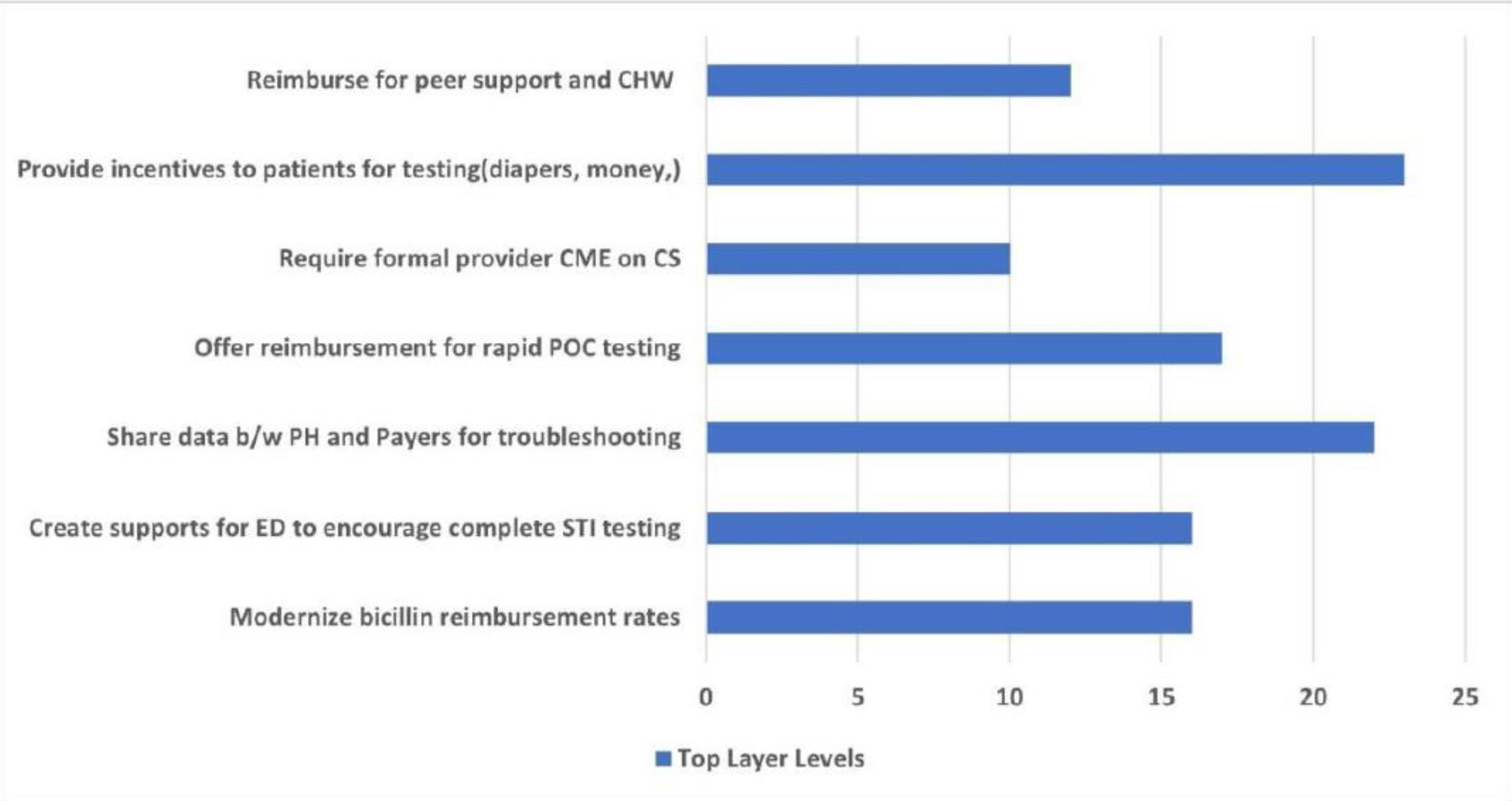
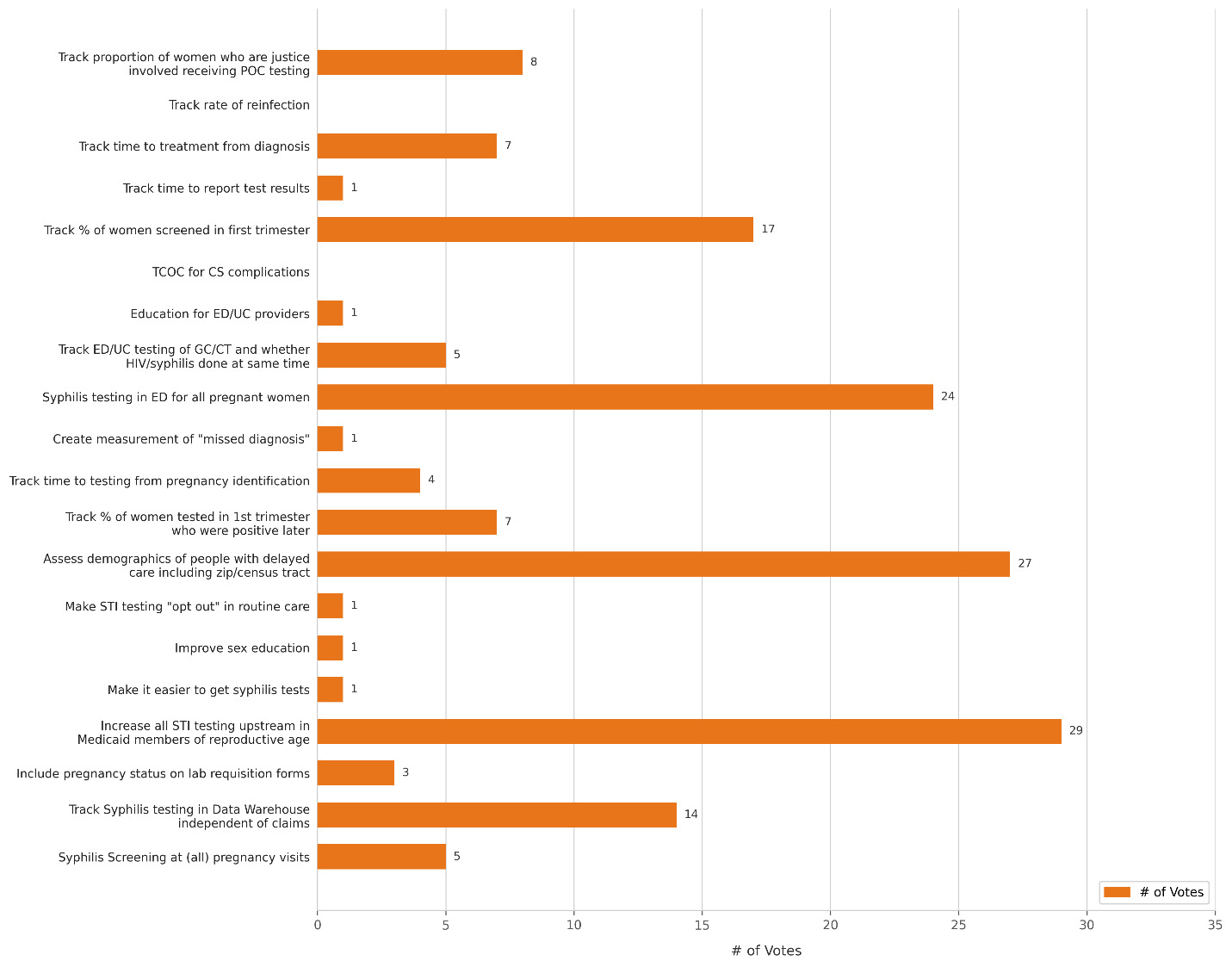
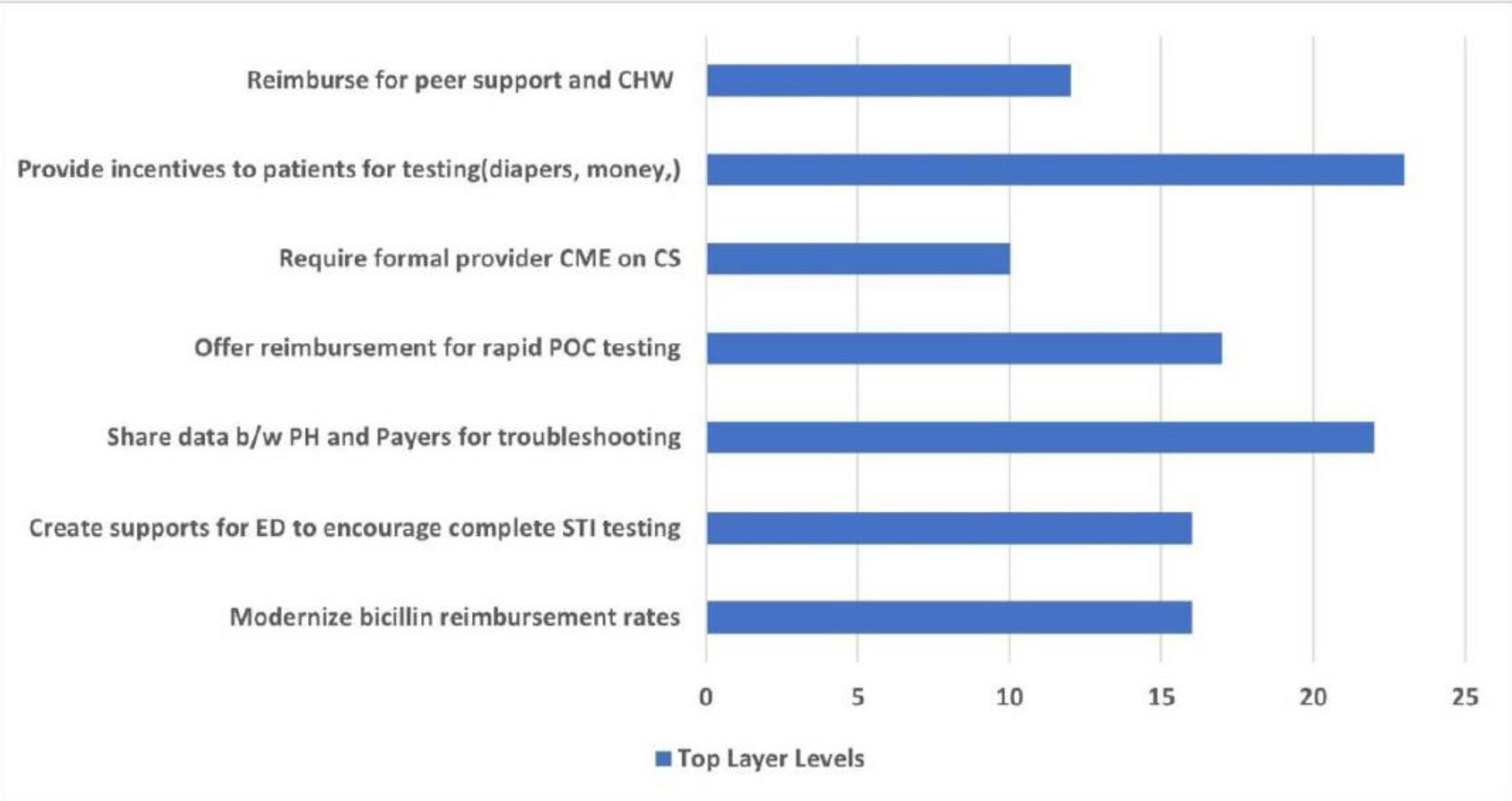
Over 30 interventions were recommended by the group of public payer and public health leaders, and 7 received the highest number of votes (Figure 2).
Finally, the group identified specific, measurable, attainable, relevant, and timely (SMART) goals with time-limited outcomes for shared accountability (Table 2). The most significant goal tied to a commitment for each state to publish shared recommendations (formed by Departments of Medicaid and Public Health) on more aggressive testing during pregnancy and identification of the birthing parent’s delivery syphilis test result prior to hospital discharge of the newborn.
Discussion
Remembering Our History with Congenital Syphilis and the US Public Health Service Study on Syphilis at Tuskegee
The first webinar and pre-summit session was an honest dialogue between a Voices of Our Fathers Legacy Foundation (VOFLF) board member, finance committee chair, and descendant of a US Public Health Service Syphilis Study at Tuskegee study participant Carmen Thorton and Milbank Memorial Fund’s President Christopher Koller, describing the historical US Public Health Service Syphilis Study at Tuskegee and the participation of Milbank in providing conditional compensation to families that experienced devastating effects from the study, particularly death. The conversation was moderated by North Carolina Department of Health and Human Services (NCDHHS) Deputy Secretary/Chief Health Equity Officer Debra Farrington, and the conversation highlighted the impact of the study on the public health community, as well as current and ongoing initiatives lead by VOFLF and Milbank in partnership to transform the tragedy of the study to one of triumph.
The lasting impact of the Tuskegee Study and similar studies continue to perpetuate distrust in US health care. Acknowledging this history was an important step and launching point. We committed to approaching this public health crisis through an equity lens, establishing the tone of the public-payer partnership by first honoring the unjust history and legacy of syphilis in the United States.
Congenital Syphilis Surveillance and Clinical Case Definitions
In the second pre-summit webinar, we invited the CDC to review syphilis and CS surveillance data across the Southeastern United States. This data dive described how the CDC measures and defines a case of CS, and the implications of this definition on downstream outcome measurements. Following this, each state public health agency was invited to share their state data, perspectives on the factors driving the increased CS rates in their states, and strategies being implemented to address these factors.
Payer Perspectives on the Congenital Syphilis Landscape
A third and final pre-summit webinar included presentations on leveraging health media in the CS campaign and current payer strategies used to drive down rates of CS in Southeastern states. Following these presentations, each state Medicaid agency was invited to present their data and current approaches for identifying and addressing rising CS rates in their states, including studies of total cost of care. Finally, Medicaid Managed Care organizations were invited to share achievements in this area. For example, one health plan highlighted regional and racial/ethnic variations in current syphilis-related claims.
The Summit
Two months after initiating the pre-summit sessions, an in-person, invite-only, day-long summit occurred that built upon the findings of the three pre-summit webinar sessions to define actions that the states were aligned to pursue. Payers and public health leaders, as well as CDC and CMS representatives, joined the active sessions of the summit, which involved creating alignment on standards of care despite great variation across national organizations and state public health laws. Participants worked on developing potential measures to allow payers to address the upstream or root causes of CS in maternity care and on identifying the most impactful and rapidly deployable payer levers that could result in a rapid reversal of CS rates. The summit concluded with the development of concrete “SMART goals” that identified solutions that attendees could support and endorse across the Southeastern United States.
Post Summit
Two virtual convenings followed the in-person summit to further refine and operationalize the agreed upon SMART goals, create shared language on the broadly endorsed testing recommendations, and create shared metrics that each Medicaid agency would collect and track. This also led to the development of a workgroup to create guidance for hospitals on CS screening policies and procedures.
The Path Forward
Historically, most states pursue priorities in the “natural silos” that exist in health care; what made this initiative unique is the partnership between public health and public payers to align and move forward together to amplify the impact of the shared priority. This is a model in health care that should be harnessed as a standard. While public health has a very mission-driven and often academic focus but little funding, public payers have ready access to financial and policy levers and a mutual desire to improve outcomes while avoiding unnecessary health care costs.
Participation in the Southeast Congenital Syphilis Payer Summit (SECSPS) required time and financial commitments; for some states, getting approval to travel for the in-person summit was not possible or prioritized. Identifying ways to prioritize these partnerships moving forward, including finding appropriate financial resources, will be critical to ensure all states can participate equally.
A collaborative framework to address these issues is essential to improve outcomes more quickly. Creating “pre-work” by setting the stage with a virtual format in advance of the summit allowed more people to participate, which allowed for a broader network to drive the momentum of the initiative. The pre-summit webinar sessions generated great interest in the summit and momentum around tackling this important public health issue. First, understanding the history of syphilis and the current state of the crisis grounded the discussion with purpose. Second, reviewing the current incidence rates across the Southeast and the stark increase compared to states in other regions of the United States underscored the importance of the convening. Third, creating a space for the sharing of ideas between commercial and public payers as well as public health organizations framed the public health issue as one that can be overcome through collaboration.
The summit participants were intentionally selected, and per state participation was limited to create an intimate “dialogue” environment. Additionally, we brought not just public health and public payer leaders, but also a variety of other national partners to incorporate their experience in the conversation. This led to rich discussions, as well as debates on what specific care gaps are causing the increased incidence of CS in the Southeast and what payer levers can be rapidly implemented to curb the rising incidence rates.
The challenge is sustaining momentum and enthusiasm to see the proposed solutions through to fruition. For example, states prepared their joint announcements on standards of testing and the importance of delaying hospital discharge until the birthing parent’s syphilis status is known soon after the in-person summit. As part of this, a “tool kit” of helpful suggestions for hospitals (Table 3) is being promoted to provide not only information about “what is best practice,” but ways to achieve best practice most consistently.
Limitations
One limitation to this initiative was the lack of funding or endorsement for state leaders to attend. In fact, both Georgia and Mississippi were unable to identify support for in-person attendance, although both states participated in the virtual pre-summit convenings. A second limitation is the identification of an “owner” to propel this work forward who can prioritize regional partnerships and identify ways to mobilize additional public health/public payer shared motivations. Each state organizes public health and public payer systems differently, resulting in a lack of a “natural” standard for the implementation of shared initiatives. Breaking down silos will look different for each state.
Future Research
Investigating how this collaborative framework can be applied to other issues, infections and chronic diseases with regional and/or national impact will be beneficial. Identifying and funding convenors who have the relationships to cross between payers and public health is an important step. Lastly, critically thinking about how and when to involve additional stakeholders such as patients and those with lived experiences will enrich the inclusive spirit of such collaborations.
Conclusion
As we move into a population health mentality and identify value-based interventions to mobilize change across large swaths of the population, pairing payers with public health leaders is critical to achieve equitable improvements in health outcomes. Funding for public health varies widely, not only within states, but across states. All payers have an incentive to avoid spending unnecessary health dollars and increase prevention and treatment strategies to improve the health of their members. Public payers stand at a unique intersection between payer and public health; the alignment of the two is critical and provides the potential for a meaningful amplification of efforts. It is essential for these two entities to deconstruct silos and collaborate to validate information, align clear messaging, and implement policies and procedures that improve the lives of those they serve. The SECSPS was organized to combat the CS crisis, and it provides a framework that can be used to tackle other current and future public health concerns.
Disclosure of Interests
The authors report no conflicts of interest or financial support.
Correspondence
Address correspondence to Brittany N. Watson, Wake Forest University School of Medicine, Department of Family and Community Medicine, 1920 W First Street, 2nd Floor, Winston-Salem, NC 27104 (Brittany.N.Watson@wfusm.edu).