Introduction
North Carolina’s immigrant population has increased dramatically over the past several decades. Since 1990, the state’s foreign-born population has grown eightfold.1 Immigrants contribute substantially to the state’s economy and civic life, including in the agriculture, construction, health care, food production, and technology sectors.2 As this population has expanded, ensuring access to responsive and culturally grounded mental health care has become increasingly important.
At the same time, immigration policy has become more restrictive and politicized. Federal and state-level policy shifts, heightened enforcement practices, and public rhetoric portraying immigrants as threats have contributed to uncertainty and fear among many families.3,4 These dynamics affect undocumented individuals, lawful permanent residents, naturalized citizens, and US-born children in mixed-status families. Mental health outcomes in immigrant communities are shaped not only by individual clinical factors but also by policy climate, social belonging, and institutional trust.
Building effective systems of care requires attention to structural determinants, access barriers, and protective community factors across the lifespan.
Policy Climate as a Determinant of Mental Health
A growing body of research links restrictive immigration policy environments to adverse mental health outcomes.5,6 State-level analyses demonstrate that more exclusionary policies are associated with increased poor mental health days and psychological distress among Latino adults, regardless of citizenship status.7 National data show that increases in immigration arrest rates are associated with worsening mental health indicators among Hispanic and Latino populations.5
These findings reflect what scholars describe as the racialization of “illegality,” in which enforcement practices and stigma extend beyond legal status and are applied broadly through racialized stereotypes.8,9 Public rhetoric framing immigrants as criminals or threats contributes to stigma and discrimination, with downstream health consequences.10
The direct mental health effects of precarious legal status are well documented. Asylum seekers and others awaiting adjudication often face employment restrictions, housing instability, limited access to services, and in some cases detention in conditions associated with trauma exposure.11 These stressors are associated with elevated rates of depression, anxiety, and post-traumatic stress symptoms.
Children and adolescents are particularly vulnerable. Family member detention or deportation has been associated with later suicidal ideation, alcohol use, and externalizing behaviors among Latino adolescents.12 Chronic exposure to enforcement-related fear can disrupt school engagement, emotional regulation, and family stability.
In this context, immigration policy functions as a structural determinant of mental health across generations.
Structural Barriers to Care
Even when individuals seek services, multiple structural barriers limit access. Immigrants are disproportionately uninsured, particularly those who are undocumented or within the 5-year federal eligibility waiting period for many public benefits.13 Although emergency care remains accessible, preventive and specialty mental health services are often out of reach.
Enforcement activity near health care settings has further eroded trust. Reports of immigration enforcement have been associated with reduced care-seeking behavior, including avoidance of needed services.14 The chilling effect extends beyond those directly targeted.
Recent federal policy changes have restricted eligibility for certain health and social supports for some lawfully present and undocumented immigrants.13,15 Such policies increase economic instability and chronic stress, both of which are associated with poor mental health outcomes. In North Carolina, workforce shortages compound these barriers.
Beyond policy, systemic gaps persist within the health care delivery system. A landscape analysis conducted by the North Carolina Institute of Medicine and El Futuro identified additional barriers, including cultural perspectives on mental health, language needs that extend beyond direct translation, legal concerns and mistrust, and a strong preference for care delivered through community-based settings.16 Together, these barriers create a fragmented system that is poorly aligned with the realities of immigrant families’ lives. Rural counties are especially affected.
Together, insurance exclusions, workforce limitations, policy restrictions, and fear of enforcement create layered barriers that delay care and reduce continuity.
Acculturative Stress and Protective Factors
In addition to structural barriers, many immigrants experience acculturative stress, defined as the psychological impact of adapting to a new cultural context. Stressors may include language barriers, economic hardship, discrimination, family separation, and intergenerational conflict.17 Such acculturative stress is associated with anxiety, depression, and somatic symptoms.18,19 Public health research has documented the “immigrant paradox,” in which immigrants often arrive in the United States with better mental health profiles than their US–born counterparts but experience declining outcomes over time due largely to acculturative stress.20
Strong family cohesion, community solidarity, faith-based engagement, and culturally rooted coping strategies have been identified as protective factors that buffer against distress.11,17 Trusting relationships with providers and continuity of care also improve engagement and outcomes.11 Effective systems of care must therefore address both risk and resilience, building on existing community strengths while reducing exposure to structural stressors.
Evidence-Based Community Approaches
Emerging evidence supports culturally adapted and community-embedded mental health interventions for immigrant populations.21–23 Culturally tailored mental health education programs are associated with improved knowledge, reduced stigma, and increased service utilization among migrant communities.21
Systematic reviews indicate that Community Mental Health Worker (CMHW)–delivered mental health interventions for Latino populations improve engagement and symptom outcomes while enhancing cultural alignment and trust.24 A randomized controlled trial of the Strong Minds Strong Communities program demonstrated significant improvements in depression and anxiety outcomes among Latino adults, with 84% having reduced symptoms of depression and 82% having reduced symptoms of anxiety.23 Improvements in psychological distress and functional disability were statistically significant and sustained at 12-month follow-up.23 Community implementation of Strong Minds in North Carolina over recent years has resulted in an even better result, with 88% having reduced depression and 85% experiencing reduced anxiety.
Community Health Workers (CHWs) frequently share linguistic and cultural backgrounds with the populations they serve. They can provide psychoeducation, skills-based support, navigation assistance, and early identification of distress while facilitating referrals to specialty care when needed.23 Training programs tailored to immigrant mental health have strengthened capacity to address trauma, acculturative stress, and stigma within community settings.25 These approaches extend the reach of specialty services and promote earlier, more acceptable points of entry into care.
A North Carolina Example: Stepped Immigrant Mental Health Care
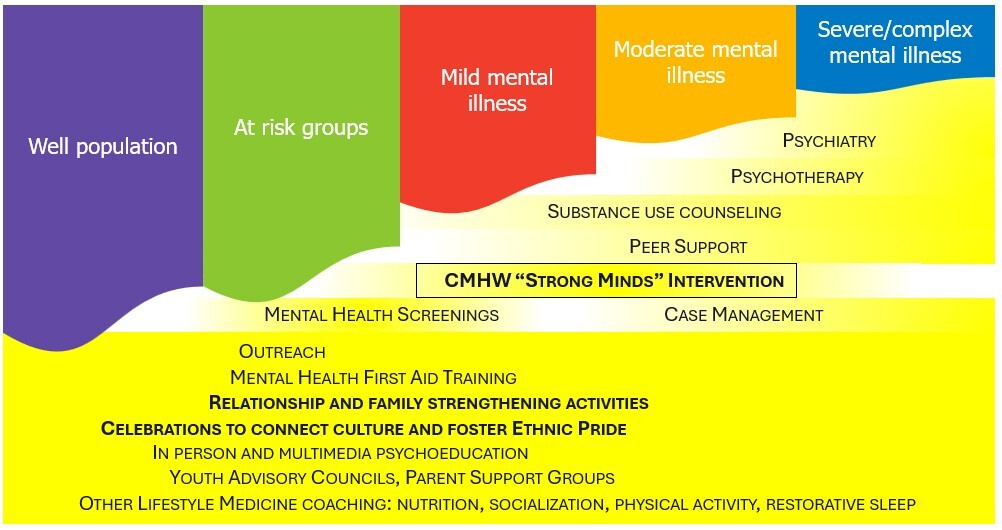
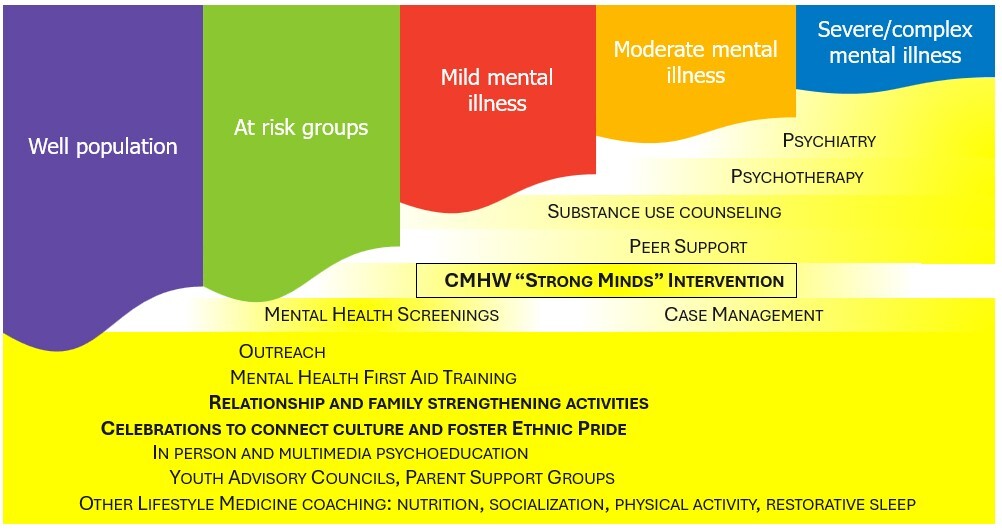
El Futuro provides a practical example of how culturally responsive, community-embedded mental health care can address persistent access gaps for immigrant populations in North Carolina through a stepped-care model (Figure 1). This approach designs culturally grounded services across the full spectrum of need, from prevention and early intervention to outpatient treatment for mild, moderate, and severe mental illness.
Founded in 2004 to serve Latino immigrant families, El Futuro initially focused on bilingual outpatient psychotherapy, psychiatry, substance use counseling, and case management grounded in family systems principles. Demand grew rapidly, reflecting unmet need and limited specialized options for immigrant communities.
Over time, it became clear that a traditional clinic-based model alone was insufficient. Workforce shortages limited the availability of bilingual clinicians, and reimbursement structures constrained expansion. More fundamentally, many individuals sought timely crisis support, psychoeducation, coping skills, and reconnection to social supports rather than long-term individual psychotherapy. Social isolation and relational disruption frequently emerged as key drivers of distress.
In response, El Futuro evolved into a relationship-centered, community-embedded organization. Group interventions, community gatherings, and culturally affirming spaces were incorporated to reduce isolation and strengthen connection. Trust was treated as a measurable outcome, assessed through engagement, referrals from immigrant community members, and retention alongside symptom improvement. Telehealth expanded access for individuals hesitant to seek in-person services due to transportation barriers or immigration-related fear. El Futuro staff and board members actively worked to address anti-immigrant narratives, identify access issues, and address health system disparities. Training opportunities for professional students and interns were made available to support workforce development.
A central innovation was the development of a stepped-care continuum anchored by CMHWs who provide the Strong Minds intervention of psychoeducation, behavioral activation, and stress management while identifying individuals who require higher-intensity services. CMHWs also conduct outreach, mental health screenings, and psychoeducational presentations in community settings. By bridging community and clinic, they reduce stigma and facilitate early intervention. Incorporation of CMHWs increased the number of immigrants served by El Futuro, reduced wait times, and allowed licensed behavioral health clinicians to see more complex cases (internal assessment of clinical data, El Futuro).
This model has demonstrated strong engagement and meaningful improvements in well-being while reducing reliance on more resource-intensive services. The model is currently being piloted statewide by the North Carolina Department of Health and Human Services, with particular promise in immigrant and rural communities. Now in its third year, Strong Minds has served more than 2000 individuals across 43 North Carolina counties.26 The intervention was developed in English, Spanish, Cantonese, Mandarin, Arabic, and Vietnamese, supporting broad dissemination.
Policy and Systems Implications
Improving immigrant mental health outcomes requires coordinated policy and systems action.
First, restoring trust in health care settings is essential. Clear protections for patient confidentiality and minimizing enforcement activity near health facilities are critical.14
Second, expanding access to preventive and outpatient services through insurance eligibility reforms would reduce untreated mental health conditions and downstream costs.11,13,15
Third, workforce investment is needed. Expanding bilingual clinician pipelines, supporting CMHW certification, and funding supervision infrastructure would strengthen capacity.11,16
Fourth, sustainable reimbursement pathways for CMHW–delivered mental health services are necessary. Evidence supports their effectiveness, yet financing mechanisms remain inconsistent.16,23,24
Finally, improved data collection and disaggregation would allow more precise identification of disparities and more targeted interventions.
Conclusion
Immigrant communities are integral to North Carolina’s social and economic fabric. However, restrictive policy climates and structural barriers create conditions that undermine mental health across the lifespan. Research demonstrates that exclusionary policies are associated with psychological distress, enforcement-related fear reduces care seeking, and children in mixed-status families face elevated risks.5,7,12 At the same time, strong family and community networks provide important sources of resilience.11,17
North Carolina has the opportunity to build trauma-informed, culturally grounded, and community-embedded systems of care. Stepped-care models that integrate CMHWs offer scalable pathways to expand access while maintaining cultural alignment.23,24
Advancing immigrant mental health requires alignment across policy, clinical practice, and community partnership. By strengthening trust, expanding access, and investing in culturally responsive workforce models, North Carolina can promote mental health equity for immigrant families across the lifespan.
Acknowledgments
Dr. Plasencia is an Executive Board Member of the Latinx Advocacy Teamwork and Interdisciplinary Network for COVID 19 (LATIN 19), a position that is voluntary and does not receive any direct financial remuneration.
The authors have no conflicts of interest or financial support to disclose.
Correspondence
Address correspondence to Luke Smith, 2020 Chapel Hill Rd., Suite 23, Durham, NC 27707 (lsmith@elfuturo-nc.org).