Introduction
On any given day, there are over 12,000 children in the North Carolina foster care system. For these children, a North Carolina district court judge has ordered that their living circumstances are so dangerous that they cannot safely live in their home with their biological family. In fact, they have been legally determined to be abused, neglected, and/or dependent based on evidence gathered by a Department of Social Services (DSS) investigation. Often, these children have experienced dozens of referrals to DSS before there are ever substantiated findings of abuse or neglect, and they are ordered to be removed by a judge. Once they are removed, if no relatives are willing or able to take them in, they are placed with a volunteer foster parent.
Imagine that you have been in a car accident that was not your fault, you have suffered a serious injury to your mouth, and you need two root canals to save your front teeth. When you arrive at your new dentist’s office, instead of finding a licensed and highly trained dentist or dental surgeon, you are told that a volunteer is there to fix your teeth. When you naturally react with fear, confusion, and doubt, you are assured that there is no need to worry and that the volunteer has had 20–30 hours of volunteer training about the subject of dental care and dental trauma. Would you even consider allowing a minimally trained volunteer to provide a specialized service that is so critical to your overall health and well-being? Of course, you would not, and you probably think it is ridiculous to even suggest it.
Children who experience foster care have significantly higher risks for mental and behavioral health issues. In fact, up to 80% of children in foster care show significant mental health challenges as compared to their peers.1 They have an increased risk of suicidal behavior, post-traumatic stress disorder, and other trauma-related symptoms. In addition, these children have higher rates of chronic physical conditions such as asthma, obesity, neurological issues, and developmental delays. They often experience challenges in school because of inconsistent attendance, and they are more likely to have learning and behavior problems.2
Child Welfare System Evolution
As the understanding of childhood trauma has evolved over time, the child welfare system structure has morphed and changed in response. Over the last two centuries, the system has gradually moved from the use of orphanages and institutional care to a much more complex system focused on permanency, safety, and well-being. Over the last 25 years, significant policy changes, particularly in funding structures, have further reshaped the system, placing greater emphasis on achieving timely permanency for children. For instance, the Adoption Assistance and Child Welfare Act of 1980 established federal Title IV-E funding as the primary source of funding support for foster care and adoption placements. This shift provided all states with equitable access to the first federally scaled funding stream to support the cost of foster care.
At the turn of the century, prevention and family preservation services were gaining increased attention, as foster care placements had been on the rise for years, and children were lingering in care. These increased pressures on the system set the stage yet again for one of the most significant federal policy reforms since the establishment of Title IV-E funding. The Family First Prevention Services Act (FFPSA) was passed in February 2018 as part of the Bipartisan Budget Act of 2019. FFPSA has several provisions that represent the most significant opportunities for systemic change in child welfare in decades. Since North Carolina implemented the legislation, changes to the use of federal Title IV-E funding have already reshaped how children and families receive services within the child welfare system. Two major areas of impact include expanded evidence-based prevention services and limitations on federal funding for certain group care placements, which, in turn, have led to the development of a new professional foster parent reunification model and new blended funding opportunities.
A Need for Prevention Services
Prior to FFPSA, Title IV-E funding could be used to supplement the costs of foster care placements for eligible children, administrative costs to run programs, staff and foster parent training, and adoption/kinship guardianship assistance. With the signing of this law, states can now access Title IV-E funding for prevention services that would allow “candidates of foster care” to remain with their families while receiving services that reduce the risk of harm and trauma. Each state had some flexibility in how it implemented prevention services; however, FFPSA outlines the criteria for prevention services eligible for this funding. It emphasizes evidence-based mental health, parenting, and substance use treatment programs. It also clarifies the length of reimbursement eligibility and service eligibility thresholds and specifies the responsibilities of the Secretary of the NC Department of Health and Human Services in administering these provisions.
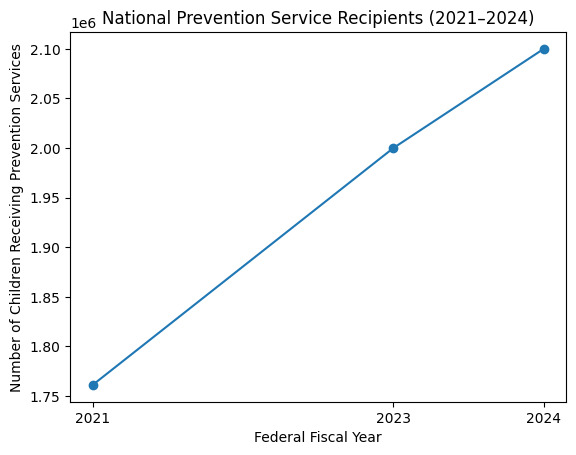
Nationally, the implementation of prevention services has increased steadily since 2021 (Figure 1). The North Carolina Department of Health and Human Services (NCDHHS) chose to implement its prevention services plan by rolling out one service at a time. The first service it chose was Homebuilders, an intensive in-home services program that works with families whose children are at imminent risk of foster care placement without the implementation of acute, intensive services focused on crisis interventions to protect children and reduce the risk of removal. NCDHHS selected regional providers to implement the service across all 100 counties. According to NCDHHS, the most recent data shows that in follow-up at six months after services end, 86% of North Carolinian children have avoided being removed from their home.3
.png)
Funding Shifts Impact the System
FFPSA changed eligibility criteria for use of federal Title IV-E funding for group care placements, limiting the funding in certain situations. Funding that was previously allotted for group care placements was reallocated to prevention services without a glide path. While idealistic in its aim to realign funding upstream and reduce long-term entries into foster care, the shift occurred simultaneously, decreasing resources downstream too rapidly, leaving gaps in resources for children already in foster care. At the same time, changes in Medicaid funding and Medicaid Managed Care implementation were beginning to reshape additional reimbursement structures for service delivery across the entire behavioral health sector. As a result, agencies across North Carolina began to reassess their service array and funding structures to establish long-term sustainability while also ensuring they were meeting the needs of their clients. An already overloaded system in crisis moved rapidly into one of the most critical and consequential periods of transformation it has ever experienced.
Children and families engaging with the system continue to face more complex and layered trauma than ever before, yet the system was never designed to meet this level of need. As a result, not only are their needs going unmet, but they are often experiencing additional harm, compounding the trauma they have already endured. The complexity of children’s needs is increasing, and the number of licensed foster homes has been declining for years, leaving children with either an under-resourced placement or no placement at all. Sibling groups are regularly separated and unnecessarily linger in care. Parents often struggle to navigate a system that can feel more punitive than restorative, and the professionals working with the families are exhausted. Traditional, volunteer-based foster care, no matter how well-intended, is not structured to meet the scale or complexity of today’s challenges. A volunteer-based model cannot carry a system in crisis. This evolving systemic complexity led to the development of the first and only professional foster parent model adopted by NCDHHS.
A Focus on Reunification as a Solution
Crossnore Communities for Children (Crossnore) developed Bridging Families as a direct response to the structural limitations of the current system. This model fundamentally challenges the assumptions of how foster care works best. Rather than presuming foster parents must be volunteers, Bridging Families positions foster parents as full-time, professional partners working alongside the birth families and their children throughout the reunification process.7 This shift is rooted in the core belief that families belong together, and that when removal cannot be avoided, every effort should be made to reunify as safely and quickly as possible.
In 2021, the model emerged as a systems intervention rooted in creativity and a willingness to question long-standing norms. Its development was grounded in research and practical application, and the model focuses not only on what is best for children and families, but also on addressing systemic barriers to reunification. The model includes a team approach where a dedicated therapist and care manager work collaboratively with the Bridge Parents and biological parents to form a team focused on healthy reunification. Very quickly, numerous funders supported the pilot’s initial expansion into Crossnore’s three primary regions. In 2024, the model was adopted by NCDHHS as the state’s only endorsed professional foster parenting model, and Crossnore launched the Bridging Families Institute to support the expansion of the model statewide.7
In the traditional system, the relationship between the birth family and foster parents is often strained or non-existent. Bridging Families takes an approach that fosters connection, mutual respect, and a shared purpose between caregivers and parents. Rather than navigating the system on their own, families are supported by an integrated team that empowers them along the way with clinical interventions and trauma-resilient tools. The model removes common structural barriers like fragmented services, inconsistent and limited visitation, and adversarial co-parenting dynamics by embedding professional parenting within a therapeutic, team-driven framework. Bridging Families is based on a dual funding model that relies on both Medicaid and Title IV-E funding to ensure sustainability.7
Bridge Parents are committed professionals who engage with the entire family throughout their journey in the child welfare system. They become part of an intentional effort to restore families. With full-time compensation, specialized training, and a team-based approach, this model minimizes foster parenting barriers and positions Bridge Parents to effectively support families on their path to reunification. This model also provides meaningful support to DSS social workers by functioning as an extension of the case planning team. The Bridging Families team works closely with DSS, sharing responsibility for family engagement, case planning, and reunification efforts. Over the next several years, the Bridging Families model will expand across North Carolina through the work of the Bridging Families Institute. The Institute provides training, coaching, consultation, and readiness support to child placement agencies committed to implementing the model with fidelity. As more agencies adopt the model, there is an intentional opportunity to transform the system from the ground up.
A Hopeful Future
North Carolina is at an inflection point in child welfare reform. Progress has been made, but a dramatic expansion of research-based services is essential to meet the needs of our state’s most vulnerable children and families. First and foremost, family stabilization and intervention programs like Homebuilders must be made available to every eligible family to prevent removal. Children need their families. If the trauma of family separation and removal can be avoided, we have a moral and ethical obligation to prevent it.
When the trauma of removal cannot be avoided, children deserve to be placed with their siblings in a setting that is designed to support the children and their biological families with integrated health and mental health services. The biological parents need coaching and mentoring that is coordinated with therapeutic and addiction recovery services to support their success. These specialized services cannot be accomplished with a volunteer workforce. Programs like Bridging Families provide professional foster parenting with integrated mental health and case management supports that wrap families in a protective network designed for their healing and success. The expansion of Homebuilders and Bridging Families into all 100 North Carolina counties must be our state’s top priority.
Acknowledgments
The authors have no financial support or conflicts of interest to declare.
Correspondence
Address correspondence to Brett A. Loftis, 100 DAR Dr, Newland, NC 28657 (bloftis@crossnore.org).