Prevalence and Need
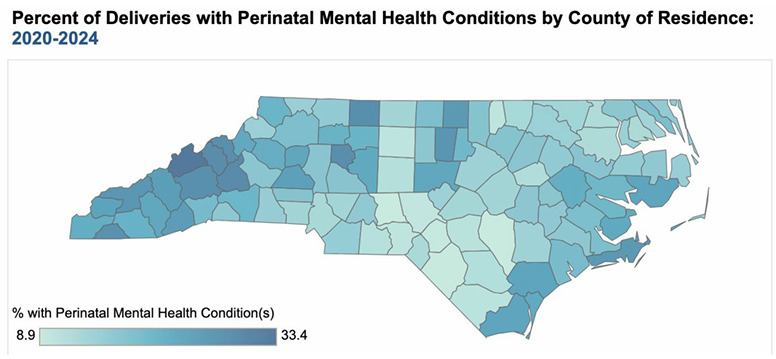
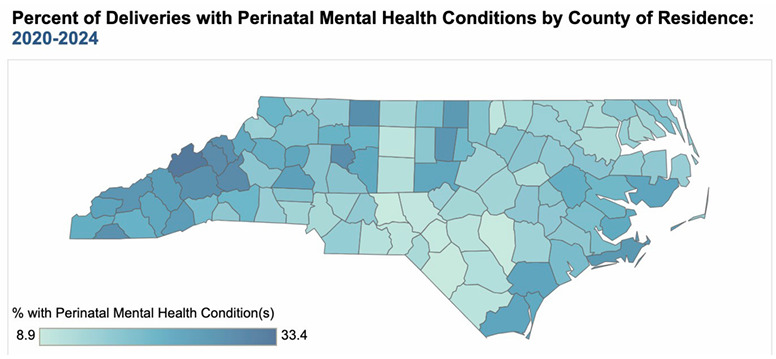
Up to one in three pregnant women in North Carolina has a mental health condition (Figure 1). Maternal mental health conditions are the leading cause of preventable pregnancy-related deaths in North Carolina.1 Nationally, perinatal depression affects approximately one in seven pregnant and postpartum individuals, which can negatively affect the health of the mother and child.2,3
Left untreated, the societal cost of perinatal mood and anxiety disorders in the United States is estimated to be $14 billion from conception to five years postpartum, with an average estimated cost of the mother-baby dyad of $31,800.4 Commercially insured women with perinatal depression were found to incur 27% higher medical and pharmaceutical spending and an average of 11 more outpatient visits than unaffected matched controls.5 Women covered by Medicaid with perinatal depression were found to have 54% higher medical expenditures and higher outpatient and inpatient utilization than women without.2
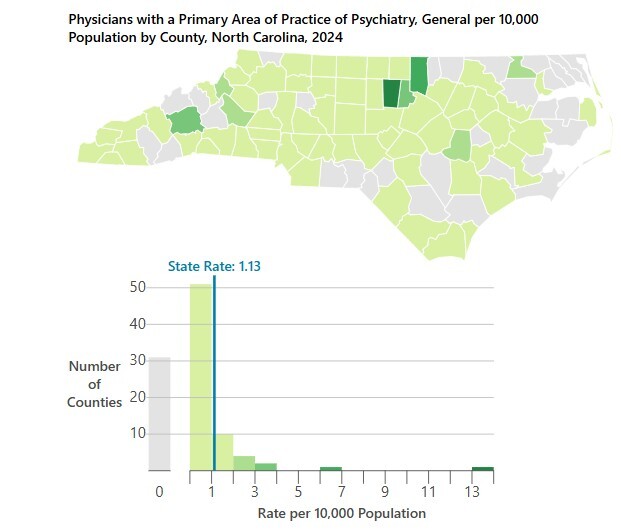
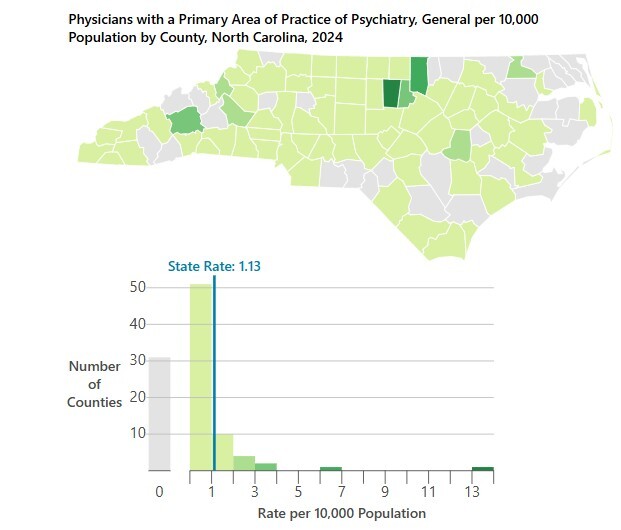
Challenges lie in pregnant and postpartum women accessing care in North Carolina, including mental health services. In the state, 20% of counties are maternity care deserts and 17% of counties have low or moderate access to maternity care.6 Additionally, there is a significant lack of perinatal mental health services in North Carolina, particularly in rural areas, with 31 counties having no practicing psychiatrists (Figure 2).
Existing Resources and Systems
In North Carolina, the importance of maternal mental health has been recognized by multiple coalitions, initiatives, and strategic plans. The NC Perinatal Health Strategic Plan and the Maternal Mortality Review Committee Report offer policy and programmatic recommendations for improvement of maternal health.7–9 The Mind the Gap coalition, led by the North Carolina March of Dimes and Postpartum Support International, is elevating awareness of perinatal mental health and advocating for increased funding to train frontline mental health providers. The North Carolina Maternal Health Innovation Program, led by the North Carolina Department of Health and Human Services (NCDHHS), is raising awareness of maternal mental health through the “I Gave Birth” campaign. In collaboration with 48 participating hospitals and providers, new mothers receive a bracelet to improve recognition of post-birth warning signs, including postpartum depression.9 Nurture NC, a backbone organization dedicated to advancing maternal and infant health across North Carolina, has identified maternal mental health as one of its priorities and is working to raise awareness of the issue and bridge connections between initiatives and programs.
Maternal mental health crisis services are available across the state and have recently been expanded. Mobile crisis teams of mental health specialists meet people in their community, and NCDHHS has launched seven new Behavioral Health Urgent Care sites, focused on supporting urgent and crisis services over the past 18 months.10 The 988 Suicide and Crisis Lifeline is a nationwide free hotline that offers crisis services and connection to local resources.11 The national Maternal Mental Health Hotline (1-833-TLC-MAMA) provides free, confidential emotional support and resources for pregnant and postpartum individuals.12 The 4th Trimester Project provides many resources for postpartum health, including mental health supports.13
North Carolina health care payers’ policies—including Medicaid, which covers more than 50% of all births statewide—support maternal health. In 2022, full Medicaid coverage was extended to women for 12 months postpartum, allowing women to access care, including mental health services, in the extended postpartum period.14 NC Medicaid covers depression screening during pregnancy and up to four times in the 12-month postpartum period. Medicaid expansion, launched in 2022, allows coverage for women beyond the postpartum period and through intrapartum periods. Through the Medicaid Pregnancy Medical Home program, a standard pregnancy risk screening form that includes behavioral health screening is required to be used by providers caring for pregnant women.15 The Medicaid Managed Care quality strategy holds Medicaid Managed Care plans accountable for elements of maternal mental health, including prenatal depression screening and follow-up.16 In addition, Medicaid, along with other payers, reimburses for collaborative care models that bring together primary care, behavioral health care managers, and psychiatry in the care of the patient.17
Evidence shows that tele-behavioral health services can improve maternal depression and anxiety, and both Medicaid and commercial insurers cover telehealth behavioral services in North Carolina.18–20 Further, North Carolina has a Statewide Telepsychiatry Program (NC-STeP) that provides infrastructure for psychiatric assessments and consultations to patients using telemedicine technologies. In July 2020, East Carolina University expanded NC-STeP to provide perinatal tele-behavioral health services in community-based rural obstetric clinics in Eastern North Carolina through the MOTHeRs (Maternal Outreach through Telehealth for Rural Sites) program. As part of this program, patients who screen positive on behavioral health screens are referred for a tele-consult with a behavioral health manager and, if needed, are referred to a tele-psychiatrist for additional follow-up. Since inception, this model has provided more than 2800 tele-behavioral health visits, saving patients 471,496 driving miles to receive psychiatric and behavioral health services.21
Through the NCDHHS Perinatal Substance Use Project, pregnant and postpartum women can reach a perinatal substance use specialist through a referral line (1.800.688.4232); the specialist provides screening, information, and connections to statewide treatment services.22 The project also maintains an updated listing of available perinatal and maternal substance use disorder residential services and provides technical assistance, education, and outreach to agencies working with pregnant and parenting women on issues related to substance use.
Perinatal substance use disorder treatment services are available through the North Carolina Perinatal Substance Use Disorder Network, a statewide, outpatient clinician-led initiative dedicated to improving access to evidence-based care for pregnant and postpartum individuals with substance use disorders. Six regional hubs—Project Cara of Western North Carolina, Sun Project and Horizons in Chapel Hill, The Tides in Wilmington and Southern Pines, ECU IMPACT in Greenville, and Cone Health’s R.E.A.C.H Maternity Clinic in Greensboro—offer integrated services that combine perinatal medical care, substance use-specific behavioral health services, medications for opioid use disorder, and wrap-around supports/care navigation.23 The regional hubs also share best practices and evidence-based clinical protocols, and they lead case consultations, quality improvement projects, policy advocacy, and workforce education. The hubs support three community spokes, have trained 50 providers, and serve all 100 North Carolina counties. Further support in outpatient settings is offered through the efforts of the Perinatal Quality Collaborative of North Carolina (PQCNC) to increase screening for substance use disorder and by Community Care of North Carolina, which developed Management of Substance Use Disorder in Pregnancy, a guide that includes recommendations for care in outpatient settings.24,25
NC MATTERS provides a free real-time consultation line staffed by perinatal mental health specialists for medical and behavioral health providers who care for pregnancy and postpartum patients.26 NC MATTERS also invests heavily in provider training and systems strengthening through their Piedmont AHEC webinar series, free clinical toolkits, a Maternal Mental Health Fellowship and annual conference, and a consultation and resource/referral phone line. They have also partnered with the NC Perinatal Substance Use Disorder Network to provide support for perinatal substance use disorder treatment.
Opportunities for Growth and Expansion
While North Carolina does have resources in place to support maternal mental health, there are significant opportunities to expand these resources. For example, the reach and utilization of existing models, like NC MATTERS and the MOTHeRS project, should be expanded.
Workforce initiatives, like those being undertaken by the North Carolina Center on the Workforce for Health, can be expanded to address workforce needs and competencies specific to maternal and perinatal mental health. Education and training of health providers on perinatal mental health and substance use disorders, including screening with validated screening tools and evidence-based treatment recommendations, should be enhanced and amplified. As one effort to address this need, the North Carolina Healthcare Association Foundation, with funding from the NCDHHS Division of Public Health, recently started new work to support North Carolina hospitals in delivering evidence-based treatments of opioid use disorder for new and expecting mothers and identifying gaps in the evidence-based care available for this high-risk population.
Additional efforts to extend maternal mental health services through innovative models of care are being launched. For example, based on the success of a program for maternal mental health developed at the Medical University of South Carolina (MUSC), H.E.A.R. 4 Mamas and Babies is a text-based screening and referral program that identifies high-risk individuals and connects them to timely and trusted behavioral health, medical, and social care throughout pregnancy and the postpartum year.27,28 In January 2026, The Duke Endowment (TDE) awarded five sites, three in North Carolina (Cape Fear Valley Health, ECU Health, and Atrium Health Wake Forest Baptist) and two in South Carolina, to implement the program. TDE plans to add additional sites as evidence is built on the replicability of this model across health systems. TDE has also funded the establishment of a Technical Assistance and Training Center, led by MUSC and in collaboration with the University of North Carolina at Chapel Hill, that will guide participating sites in program implementation and lead evaluation activities.
Other opportunities exist for increasing access to care, including in rural maternity deserts. One such model is a shared maternity care model.29 In this model, primary care providers (usually family medicine physicians) in the local community provide prenatal care, and another health care provider (usually an OB-GYN) sees the pregnant women periodically during the pregnancy and for delivery. The patient can continue their relationship with their local primary care provider and continue any behavioral health support they may be receiving in the primary care home. The American College of OB-GYN and American Academy of Family Physicians have a joint statement supporting collaborative maternity care services.30 This model of care could be extended by providing in-home care and mobile units.
There are multiple other examples of innovative perinatal care models emerging nationally that have evidence of improving maternal mental health. These could be adopted in North Carolina. For example, Pomelo Care provides virtual 24/7 preventive care, behavioral health screening and support, and primary care services through 12 months postpartum. This model reports that engagement with the program is associated with a 1.7-fold increase in mental health screening rates.31 Cayaba Care (now known as Nadia Care) provides comprehensive in-person and virtual wrap-around support throughout pregnancy and postpartum and reports that engagement with the program is associated with a 56.5% decrease in postpartum depression rates.32 Ouma Health is a dedicated maternity telehealth platform led by maternal-fetal medicine physicians that provides clinical care, including psychiatric nurse practitioners who manage mood disorders in perinatal patients and addiction medicine specialists who provide medication-assisted treatment for substance use disorders. Within the first six months after its launch, Ouma announced that 27% of the patients were diagnosed with previously unrecognized depression and escalated for a visit with Ouma’s behavioral health team.33
Maternal mental health is also affected by factors outside of the medical model; a wide range of social factors and unmet social needs, including economic and food insecurity, have been linked to adverse maternal mental health outcomes.34–36 Economic supports have been shown to improve maternal mental health, along with other positive effects. Public food assistance, like the Supplemental Nutrition Assistance Program (SNAP), may reduce maternal depression.37,38 A refundable state Earned Income Tax Credit has been found to reduce maternal stress and depression.39 Cash transfers have been shown to improve maternal mental health.40 Rx Kids, a prenatal and infant cash transfer program recently expanded in Michigan, has been shown to reduce maternal postpartum depression, stress, and anxiety.41 The Bridge Project, a similar prenatal and infant cash transfer program active in 12 states, reports that 88% of enrolled mothers reported improvement in mental health and stress.42
Efforts to advance the above policies and pilot programs, as well as many others that are not mentioned, are underway in North Carolina. Finally, while North Carolina does have programs in place and opportunities for expansion, we do not have a connected, comprehensive maternal mental health system. It is fragmented and we can, and must, do better by creating interconnectedness in the system to optimize existing and new resources.
Conclusion
Maternal mortality and morbidity rates continue to rise, especially among minority and rural populations, and mental health conditions are the leading cause of preventable pregnancy-related deaths. Maternal mental health is fundamental to women’s health and the health of infants and families. Maternal mental health begins before a woman becomes pregnant and lasts well after delivery. Resources need to be made available, in a coordinated and longitudinal way, throughout a woman’s life. North Carolina has many strengths and resources to support mothers, but further investment in and coordination of those services is needed to meet the needs of our population.
Acknowledgments
The author is financially supported by the HopeStar Foundation and reports no conflicts of interest. The author is grateful for the input on this commentary from many professionals leading the identified programs.
Correspondence
Address correspondence to Elizabeth Cuervo Tilson, 428 East 4th St, Suite 408, Charlotte, NC 28202 (betsey@nurturencnow.org).