Context for Alarm and Reform
Almost five years have passed since the U.S. Surgeon General issued a national advisory on youth mental health.1 The report described increases in the prevalence of youth mental health disorders in the context of the social disruption associated with the COVID-19 pandemic and the risks associated with the use of digital technology. The report garnered attention by acknowledging the crisis that many families were already experiencing. For many in North Carolina, for example, the unmet youth mental health needs described in the advisory were not new.2 Our state has pursued mental health reform for more than a quarter century, with repeated efforts to strengthen community-based care while controlling costs. Across this long arc of reform, partners at every level (e.g., legislators, state agencies, health systems, schools, community providers, and family advocates) have invested enormous energy in planning and reforming the system. However, the defining experience for many families and providers has been instability and uncertainty rather than coordinated reliable support.
How can the system be so unpredictable when 94% of North Carolina youth have health insurance and 93% of eligible children participate in Medicaid?3 Efforts to “transform” Medicaid Managed Care have so far proven inadequate to ensure meaningful access to care (e.g., no improvements in rates of well-child visits or follow-up for children prescribed attention-deficit/hyperactivity disorder [ADHD] medication), and worse, they may have created more barriers to accessing services through administrative burdens.4 Many insured families who need mental health services for the first time are surprised when they are placed on waiting lists for months or told to go to the emergency room for care. Families are asked to find an elusive “front door”; they confront varying eligibility pathways and inconsistent language around services and coverage.
What most families do not see is that behind the scenes, providers have been scrambling to adjust to constant structural change and administrative demands. Authorization rules and billing portals shift just as clinics gain traction delivering treatment. Provider networks are reconfigured, then reconfigured again, triggering new contracts and credential requirements. Documentation standards change, often with good intentions, but the cumulative administrative lift diverts time from care and quality improvement. Reimbursement rates change while the workforce shrinks. Data are siloed, limiting our ability to monitor access, continuity, safety, and outcomes across the multiple settings where young people receive care (e.g., home, school, primary care, community programs, crisis services, child welfare, and juvenile justice).
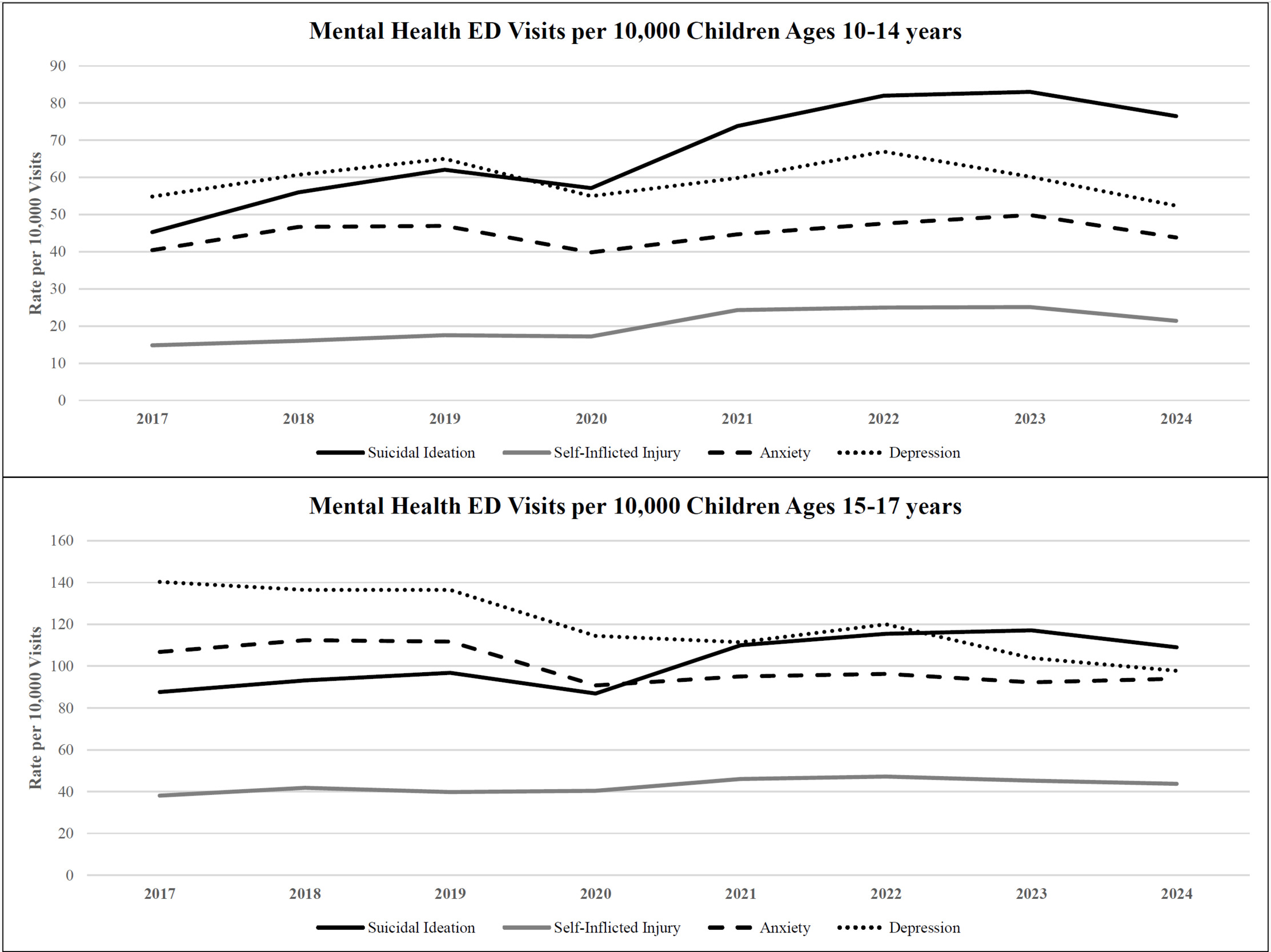
Recent data underscore the paradox of constant motion without clear improvement. Each year, parents in North Carolina respond to a question on the National Survey of Children’s Health asking about their experience trying to access mental health care for their child. The proportion of parents who reported that it was difficult or impossible to get treatment for their child has increased from 48% in the 2021–2022 survey to 55% in the most recent 2023–2024 cycle.5,6 Accordingly, from 2017 to 2024 the state rate of child emergency department (ED) visits for self-inflicted injury have increased by 31% (from 11.2 to 14.7 per 10,000 ED visits), and the share of visits for suicidal ideation have increased by 47% (30.2 to 44.3 per 10,000 ED visits).7 Figure 1 displays the rate per 10,000 ED visits for specific mental health diagnoses, with separate charts for children aged 10–14 years and youth aged 15–17 years, captured by the North Carolina Disease Event Tracking and Epidemiologic Collection Tool (NC DETECT).
_visits_for_youth_by_age_group_and_condition__2017-.png)
ED visits for children’s mental health concerns continue to occur despite widespread agreement that most emergency rooms are not equipped to manage mental health conditions, that treatment in the ED may worsen symptoms, and that reducing ED visits for youth is an achievable goal.8,9 The trends are noticeable for at least two reasons. First, after 2020, rates of suicidal ideation have increased dramatically, and most noticeably for early adolescents; second, the trends are noticeable for the general stubbornness of these rates over the past two decades.7,10 Taken together, ongoing system transformation, persistent barriers to accessing community-based mental health treatment, and rising rates of mental health-related ED visits suggest a pattern: a system that is highly active, but not yet delivering timely, effective, or developmentally appropriate care.
How does this play out at the family and community level? Anecdotally, two consistent patterns have emerged. First, consider a small regional clinic delivering evidence-based treatment for adolescent anxiety and depression. The leadership supports clinician training and supervision, invests in fidelity monitoring, and builds referral pathways from schools and pediatric practices. As workflows stabilize, payer rules shift, network alignments change, prior authorization criteria update, and reporting templates change. The clinic pauses, recalibrates, and loses momentum. Staff are lost, turnover occurs, and the team returns to square one. Second, consider parents of a struggling teenager. The family gets inconsistent advice from various sources (e.g., a school counselor, pediatric provider, online resources), each with partial information on insurance, service availability, and treatment plans. Without clear next steps, confusion and helplessness persist, possibly causing more conflict and delays in care. Families do not need perfect uniformity; they need dependable pathways, timely access, and continuity when the care setting or intensity changes. Community providers want a coordinated care system to assist.
The Path Forward: Stable but Continuous Improvement
What would it take to move to a stable high-quality system without triggering another wave of disruptive reforms? A pragmatic approach centers on steady structures and shared learning. The core idea is simple: strengthen the system we already have by reducing unnecessary variation, invest in infrastructure for community learning and improvement, and align incentives so that prevention and early intervention are the priority. This suggests a clearly defined and adequately funded statewide coordinating entity responsible for communication, oversight, and accountability across the system. This is an argument for consistent rules of the game, transparent feedback loops, and practical support for providers and families who experience the system most directly.
North Carolina does not have to build this system from scratch. A promising example of clarity in vision and outcomes is the North Carolina Division of Mental Health, Developmental Disabilities, and Substance Use Services (DMHDDSUS) Strategic Plan for 2024–2029.11 The plan, recently updated with a Year 1 Annual Report and accompanying dashboard, sets clear priorities and tracks over 30 measures.12 By maintaining a stable set of metrics over multiple years, it models the type of time-consistent accountability that enables system learning.
However, only a handful of measures focus on children’s mental health and are designed to monitor restrictive settings (e.g., “Number of Medicaid children with mental health needs held in an ED or boarded in a Department of Social Services [DSS] office”; “Number of children served in an out-of-state Psychiatric Residential Treatment Facility”). Additional measures are needed to assess access to care, the quality of community-based care, and ultimately, improvement in child symptoms. To be successful, the plan must be aligned with other areas of the system that influence youth mental health, such as North Carolina’s Medicaid and child welfare systems.
Medicaid transformation provides a substrate on which DMHDDSUS’s strategic priorities and measures can align. Medicaid Managed Care Organizations are the central actors in the child mental health system. Importantly, as of December 2025, the state is implementing a Managed Care plan for youth in foster care, the Child and Family Specialty Plan (CFSP).13,14 While this represents another major system realignment, the CFSP is a desperately needed statewide plan for youth in foster care, who represent a small proportion of the population yet account for a disproportionate share of high-acuity services such as residential treatment. Managed Care plans like the CFSP offer an opportunity to replace costly, reactive services with family-centered preventive care, promising stable care management, evidence-based treatments, and better coordination among child welfare, schools, and community providers. Every community should know exactly what the Managed Care plans in their region are doing. Every child welfare worker should know exactly what the CFSP plan is doing for youth in foster care in their county.
Medicaid Managed Care transformation may enable value-based payments to enhance collaboration rather than competition. Well-designed models can reward access and outcome improvements without penalizing providers or plans during challenges. As children’s mental health relies on families, community providers, schools, and Managed Care Organizations, value-based payments should benefit all partners. Successful reform may also need a managing authority for consistent communication, shared standards, and coordination among all entities implementing system changes. One example that the state can look to scale statewide is the NC Integrated Care for Kids (NC InCK) program, which is an ambitious partnership across five counties that has leaned into this challenge.15,16 NC InCK offers whole-person care, leverages multi-sector data to identify families for enhanced care management, integrates services across systems, and links payments to providers based on performance on core measures.
Conclusions
The system is only as strong as its weakest link. Youth mental health cannot be separated from the broader landscape of child well-being. The challenges we see in the mental health system often originate upstream in the systems where young people spend most of their lives. When schools are under-resourced, when student support personnel are stretched thin, or when children experience instability in foster care, those pressures surface in emergency departments, crisis services, and residential treatment. Weaknesses in child-serving systems are not simply adjacent to the youth mental health system; they become part of it. Sustainable improvement will require coordinated action with schools, early childhood programs, child welfare agencies, and family support systems, aligning mental health policy with the broader conditions that allow children and families across the state to thrive. Clear identification of a well-supported statewide entity responsible for guiding implementation, aligning standards, and ensuring accountability across sectors would better position effective mental health policy within the broader context in which children and families across the state thrive.
Public–private partnerships will determine our trajectory. Managed Care Organizations, health systems, and technology companies can feel like outsiders in a publicly financed system. Yet, private partners also bring tools—analytics, product design, and human-centered technology—that can complement and amplify the reach of public systems. The lesson is not to embrace or reject corporate actors wholesale, but to demand public value: set clear expectations, ensure transparency, align incentives to outcomes that matter to families, and use procurement and contracting to foster shared learning and improvement.
Three principles guide the next phase. First, the system must commit to smart stability. North Carolina’s youth mental health system needs a stable rule set for improvement. Second, we should build a shared learning infrastructure for collaboration. This involves establishing persistent measures, coordinating privacy-protected data sharing, and investing in learning collaboratives. These tools align the work of families, providers, schools, and Managed Care Organizations around outcomes that matter to diverse families statewide. Third, we need to strengthen community-based care. Access depends on clear, simple front doors, timely evidence-based treatments, smooth transitions, and practical workforce support. State leadership can reduce administrative friction, invest in local capacity, and ensure that community providers and youth-serving systems have what they need to deliver dependable care close to home. Measurement should be modest but meaningful. Rather than dozens of shifting indicators, the state can commit to a consistent scorecard featuring measures that matter to families and providers (e.g., time to first appointment; proportion receiving evidence-based treatment; 30-day follow-up after crisis; continuity between care settings; family-reported navigation experience). Crucially, the scorecard should persist across contract cycles and leadership changes so that trend lines tell a trustworthy story.
To translate measurement into improvement, North Carolina can seed regional learning collaboratives that bring together schools, community providers, Managed Care entities, pediatric practices, and family advocates around shared aims and data.16 The UNC Carolina Across 100 CARE4Youth project is an example of how to support local teams to build and sustain collective improvements.17 Similar to NC InCK, scaling this initiative from 18 counties to the entire state is today’s challenge and requires leadership to recognize and foster flexible but disciplined growth.
It is important to acknowledge genuine progress. Attention to youth mental health has expanded across sectors, partners have invested in workforce, training, and telehealth capabilities, and communities have developed creative responses that fit local context.12,18 Perhaps we do not need to elevate innovation as the highest value right now; we may need to focus on stability and maintenance. This may seem counterintuitive in a time that demands urgent action and prizes novelty. First, we need to ensure that every community has reliable access to the things we already know work. The next phase, defined by stability and continuous improvement, would allow the best ideas to travel and the gains to endure.
Acknowledgments
The author would like to thank the following individuals who provided feedback on drafts of this commentary: Mark Holmes, Helen Newton, and Max Shafir.
Financial support
The author has received funding from the NC Department of Health and Human Services to implement and evaluate mental health programs. The opinions expressed in this commentary are those of the author and do not necessarily reflect the views of the funding agency.