

Introduction
Digital technology has surged in popularity in recent years, with health care systems incorporating virtual connectivity and platform interoperability to strengthen access to care and promote health equity. Such efforts have been particularly true in medically underserved and rural regions, where a confluence of factors including health care and specialty provider shortages, transportation barriers, geographic limitations, disproportionate rates of disease burden and chronic illness, socioeconomic challenges, care stigmatization, and hospital closures have historically impeded quality access and timely care provision. In Eastern North Carolina, a 41-county region east of the I-95 corridor, nearly 50% of the catchment area is considered economically distressed and is, relative to other regions across the state, one of the poorest.1–3 Residents within this region encounter poorer chronic disease outcomes, experience higher mortality and morbidity rates, and frequently face long travel distances to hospital-based care and specialty services.1 When considering ways these factors impact rural youth, data is equally as stark.
In Eastern North Carolina, rural youth experience higher rates of mental health crises, obesity, and substance use, potentially elevating risk for development of a mental health disorder compared to non-rural peers.4 While more recent NC Healthy Schools Youth Risk Behavior Survey data suggest improved emotional health among North Carolina youth, many agree that the state continues to face a youth mental health crisis. In 2021, over 1 in 10 children aged 3–17 reported receiving a depression or anxiety diagnosis, and 1 in 10 high school students reported a suicide attempt.5 While need is evident, factors like mental health workforce shortages and the paucity of youth-focused treatment options, particularly in rural areas, have left 72% of youth struggling with a treatable mental health disorder without care.5,6 These challenges underscore a significant unmet need and catalyzed the development of Healthier Lives at School & Beyond (HLSB), a school-based telehealth program expanding access by delivering services where youth are most consistently present—within schools—while reducing structural barriers through virtual care. This article provides an overview of HLSB’s integrative school-based care approach and specifically explores behavioral telehealth services.
Program Overview
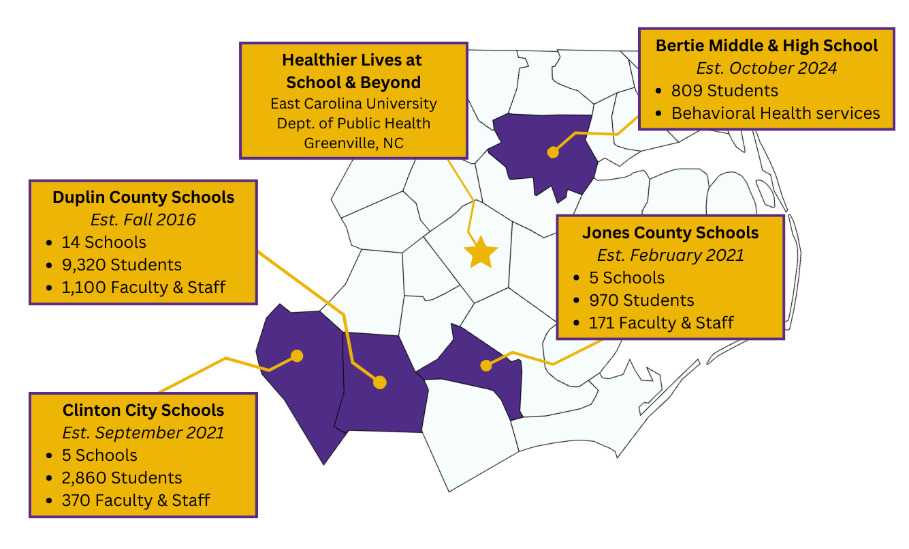
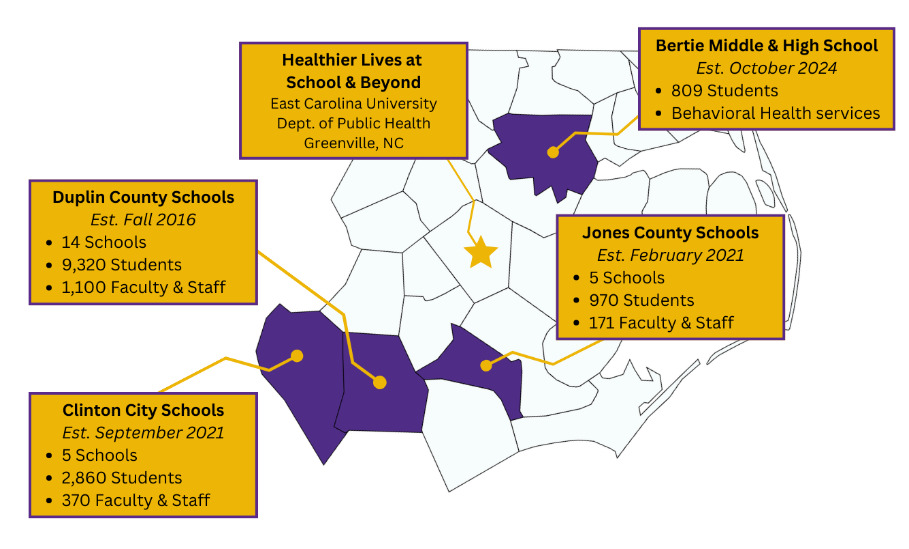
In 2016, during its initial planning phase, the HLSB program was designed to replicate the model of a traditional school-based health center while innovating by delivering services remotely within schools, an approach that was largely uncharted at the time. This delivery model allowed for a team of multidisciplinary health care professionals practicing within a regional academic medical center—the Brody School of Medicine (BSOM) at East Carolina University (ECU)—to provide real-time nutrition counseling, behavioral health, and acute medical services to students, faculty, and staff in rural school districts. Initially piloting in three initial schools, as shown in Figure 1, the HLSB program has since expanded to include 26 public schools (pre-K–12) across four rural Public School Units (PSUs) in Eastern North Carolina. Communities within this catchment are designated as Mental Health Professional Shortage Areas and are collectively home to over 13,300 enrolled students and 1745 employed school faculty and staff.1,7
In response to regional needs, the HLSB program is guided by objectives that include enhancing access to care, preventing adverse effects of chronic disease, reducing student absenteeism, and minimizing unnecessary emergency department visits. Additional goals include improving educational outcomes and supporting school faculty and staff through worksite wellness initiatives, such as virtual support circles facilitated by HLSB behavioral health providers during the COVID-19 pandemic. Since program inception, over 6000 telehealth encounters have been completed across all HLSB service lines, including acute medical, nutrition counseling, and behavioral telehealth services.
Multidisciplinary care
Given the magnitude and multidimensionality of HLSB program objectives, compiling a team of professionals from various health care domains is essential. Although school-based studies examining the efficacy of multidisciplinary care approaches are still emerging, broader health care research shows that multidisciplinary care teams in non-hospital and community settings improve patient-reported outcomes (such as care satisfaction and self-efficacy), enhance care coordination, and contribute to better social-emotional health.8–10 Multidisciplinary care teams, by definition, are collaborative groups of professionals representing multiple disciplines who coordinate assessment, planning, and service delivery of specific populations.8
Within the context of the HLSB program, multidisciplinary care team members include licensed mental health providers, registered dietitians, board-certified pediatricians, and advanced care providers, as well as graduate-level behavioral health and nutrition interns, medical students, and internal medicine/pediatric residents. The team works in tandem with multidisciplinary school supports at each originating site (schools), including HLSB-employed, community-based support staff and telehealth logistics coordinators (TLCs). These “boots-on-the-ground” team members assist with community outreach, provide on-demand, on-site school support, tele-present students, attend School Health Advisory Council (SHAC) meetings, and bridge communications between clinical HLSB and school support staff. Appendix A presents a full list of multidisciplinary care team members.
External community-based supports (outpatient mental health therapists, caseworkers/child protective service agencies, primary care providers/pediatricians, health department providers) and pre-existing in-school supports (co-located school-based mental health providers, other virtual school-based telehealth providers, community organizations running in-school support programming) are also incorporated into shared care planning and coordination efforts with proper consent. These approaches have contributed to:
Timely access. HLSB providers have the option of referring care to one another after a student is established with the program and co-morbidities are identified.
Shared treatment planning. HLSB providers have a shared record system and can ensure a tailored treatment approach that integrates the whole child and whole health.
Improved system-level collaboration between health care, family, and school. HLSB providers actively utilize the Centers for Disease Control and Prevention’s Whole School, Whole Community, Whole Child (WSCC) framework to inform coordinated care efforts.11
A non-HLSB-affiliated pediatrician working within a rural county served by HLSB services described their experiences with HLSB’s care approach:
“You just overcome all [the rural health] barriers in one fell swoop. And when I have a child who needs something, I know I can get the child to services. Every person that I have sent to a nutritionist or behavioral health specialist [via telemedicine] has been a success story. Their lives have been touched and changed by it, and they have been made healthier by it. And having children who are physically healthy, mentally healthy, and nutritionally healthy creates stronger communities.”
Overview: HLSB Behavioral Telehealth Services
Research suggests that schools have increased access to mental and behavioral health more than any other setting, and nearly one-third of adolescents who receive mental health services do so exclusively within an academic space.12,13 PSUs served by the HLSB program are categorized by the Health Resources and Services Administration of the U.S. Department of Health and Human Services as Mental Health Professional Shortage Areas (MHPSAs) and are five times less likely to have access to a qualified mental health provider.1,14 To address this need, HLSB behavioral telehealth services are designed to: 1) provide early identification and intervention support for common pediatric mental health needs/complications; 2) provide high-quality student- and family-centered behavioral telehealth services grounded in evidence-based practices; and 3) collaborate with PSUs on tailoring behavioral telehealth service integration that builds upon and compliments pre-existing student support services and frameworks, such as multi-tiered systems of supports (MTSS).
Components of Care and Workflow
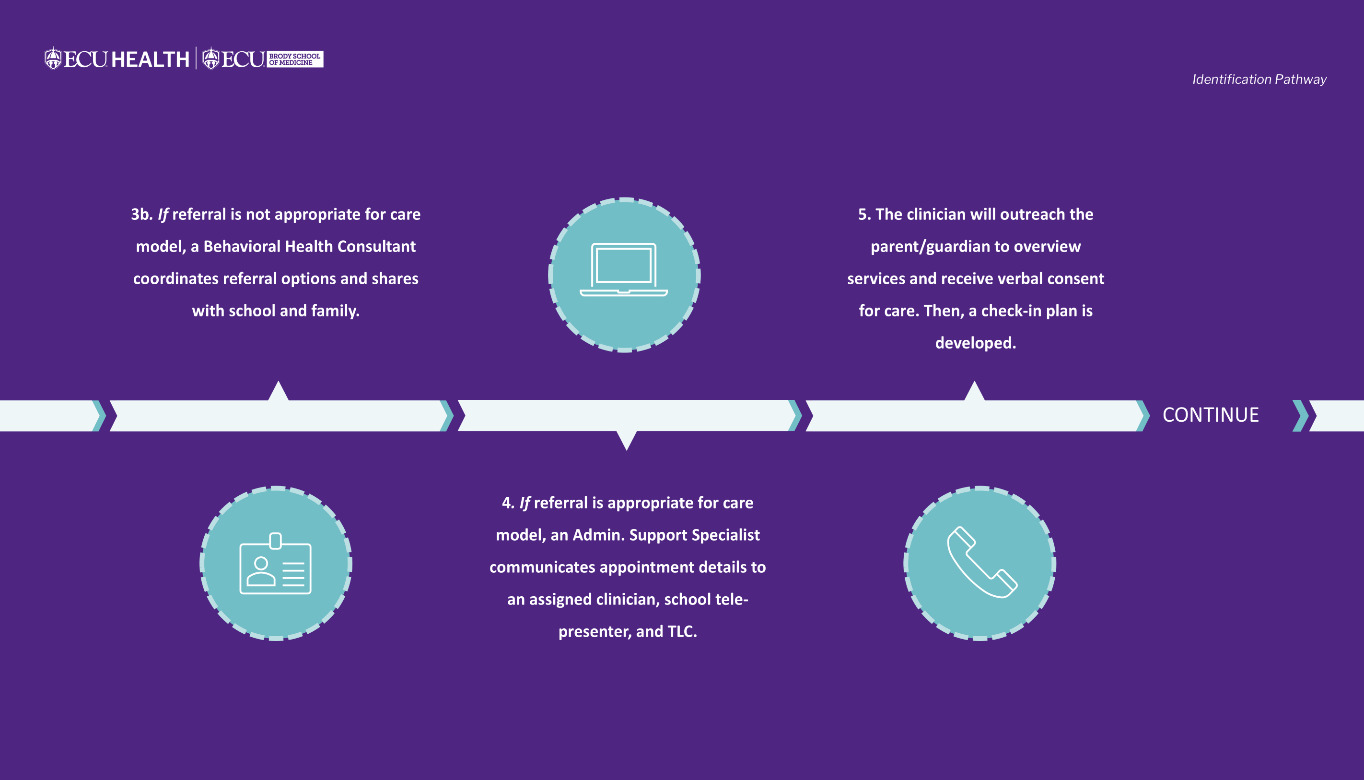
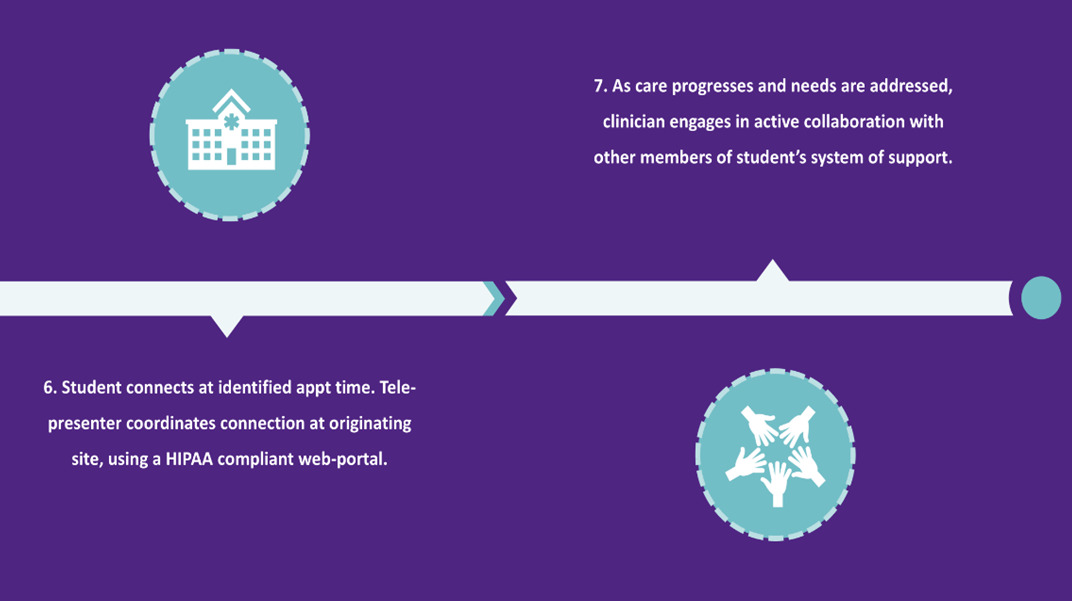
Behavioral telehealth services offered within the HLSB program are designed to improve access to evidence-based pediatric mental health treatment by virtually connecting licensed mental health providers or graduate-level clinical interns to patients presenting with mild to moderate behavioral health concerns necessitating clinical intervention and support. By providing these services virtually, traditional access barriers are eliminated. Services are delivered using synchronous, real-time, HIPAA-compliant audio-video technology in a private environment within the school. The HLSB program provides tablets at each school to facilitate telehealth connections, with appointments scheduled during non-core instructional periods (e.g., encore or resource time).
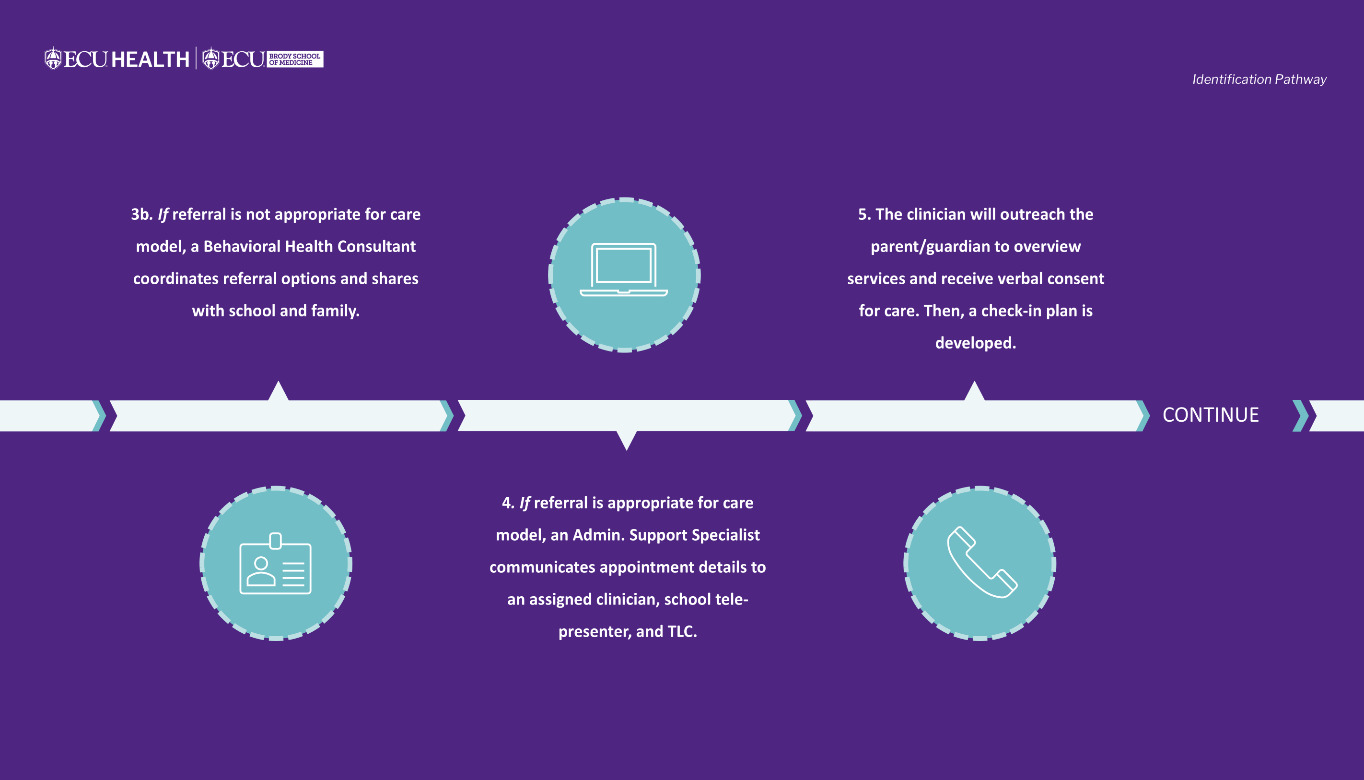
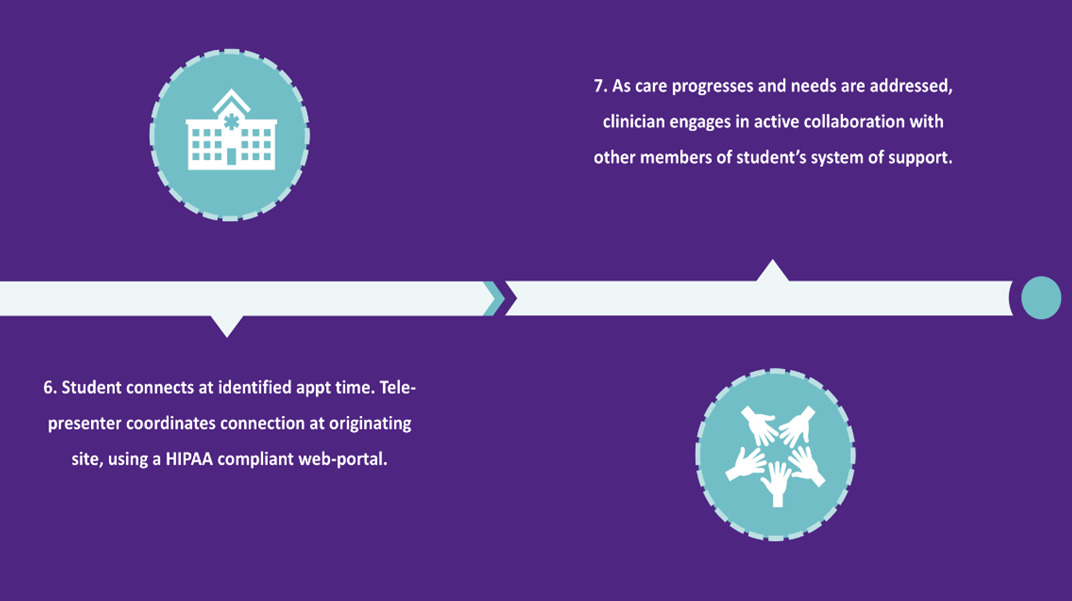
To replicate the in-person therapeutic environment, schools are also supplied with items that promote warmth, safety, engagement, and self-regulation during virtual visits. These include stress balls, fidgets, textured tactile stickers, pop-it toys, finger puppets, feelings games, materials to support artistic expression and dramatic play, and a treasure chest from which patients choose a treasure at the conclusion of each appointment. Additionally, schools are provided with copies of frequently used, validated pediatric screening tools, including the Patient Health Questionnaire-Adolescent (PHQ-A), Pediatric Symptom Checklist (PSC-17), Screen for Child Anxiety Related Disorders (SCARED), Vanderbilt Assessment Scales, and Child PTSD Symptom Scale (CPSS); they also have safety plan templates with local crisis resources for use at the clinician’s direction. Figure 2 presents a visual overview of the program’s referral-to-care workflow.

Evidence-Based Practice
Behavioral telehealth services are delivered within a brief, time-limited care model (6–12 bi-weekly psychotherapy sessions, with a 30–40-minute duration) appropriate to the school setting. Interventions emphasize targeted skill development, symptom stabilization, and coordination with families, the school, and community providers when longer-term or specialized care is warranted.15 Behavioral assessment and psychotherapeutic interventions are grounded in evidence-based theoretical frameworks and theories, including brief cognitive behavioral therapy (B-CBT), solution-focused brief therapy (SFBT), motivational interviewing, problem-solving therapy, dialectical behavioral therapy (DBT), and family systems theory. Therapeutic techniques and interventions are developmentally tailored to meet the developmental, contextual, and biopsychosocial-spiritual (BPSS) needs of patients and their support systems.
Multi-Tiered System of Supports (MTSS) Integration
Behavioral telehealth services are integrated within existing school-level support structures to facilitate coordinated, individualized care grounded in a whole-child framework (e.g., WSCC). In alignment with MTSS prevention and tiered service delivery principles, interventions emphasize early identification, promotion of student well-being, academic success, social-emotional functioning, and family engagement.16 Referrals for behavioral telehealth most commonly correspond to Tier 1 (universal) and Tier 2 (targeted) supports, with a smaller proportion reserved for students demonstrating Tier 3 (intensive) needs.17
Common Referral Reasons
Students are commonly referred for concerns including anxiety, depressive symptoms, adjustment-related difficulties, neurodevelopmental conditions, disruptive behavior disorders, trauma, and grief. Diagnostic patterns of students (aged 5–12 and 13–19 years old) served during the previous academic year (school year 2024–2025) largely reflected these presenting concerns, with the five most frequent diagnoses summarized in Table 1. The most frequently assigned DSM-5-TR diagnosis was Z71.9 (Other Counseling or Consultation), reflecting the program’s emphasis on early identification, brief supportive interventions, and skill-building to promote student well-being while avoiding over-pathologizing normal developmental and adjustment challenges.18 Other common diagnoses, including anxiety, depression, and adjustment-related and trauma disorders, illustrate the program’s responsiveness to a range of behavioral health needs (Table 1).
Training and Education: Behavioral Telehealth Interns
Given persistent shortages in rural mental health care, a concurrent goal of the HLSB program is to train, prepare, and equip graduate behavioral health learners to meet the needs of underserved rural populations, strengthen skill in virtual pediatric telehealth practices, and help fill the rural workforce provider pipeline. Graduate interns represent disciplines from across ECU’s campus, including pediatric school psychology (PhD), clinical health psychology (PhD), clinical counseling (MS), counselor education (MS), and marriage and family therapy (MS), and make up 60%–70% of the overall HLSB behavioral health team annually. Licensed mental health clinicians, who dually serve as faculty and staff at the Brody School of Medicine, provide direct clinical supervision to graduate interns completing basic and advanced practicum requirements with the HLSB program. Since becoming an official clinical internship training site in 2020, HLSB has trained over 30 ECU graduate students, with 99% indicating a satisfactory or extremely satisfactory clinical experience.
Conclusion and Reflections
Delivering behavioral telehealth services in rural school settings maximizes reach, minimizes barriers, and ensures that interventions occur in a familiar, supportive, and collaborative environment. Programs like HLSB have potential to serve as a replicable program model as state-wide youth mental health initiatives move toward advancing school-based behavioral health programming and infrastructure. For example, state legislation passed in 2020 (SB 476) sought to enhance mental health support available in K-12 schools; in 2023, the North Carolina Department of Health and Human Services, in partnership with the North Carolina Department of Public Instruction, developed a state-wide School-Behavioral Health Action Plan including investment proposals supporting school-based telehealth pilot programs.19,20
As the integration of telehealth and school-based health care continues, there is also a need for interconnected research, policy, and practice agendas on state, regional, and local levels. Groups like the Collaborative for the Advancement of School Telehealth are aiding these efforts, creating a consortium of school-based telehealth programs from across the Carolinas, Georgia, and Virginia where shared learning, research, and program sustainability planning can convene.21 No matter what the next direction of school-based telehealth services is, one thing is certain: for as long as it can, HLSB will continue to bridge barriers and support rural youth one telehealth connection at a time.
Acknowledgments
Our sincerest thanks to Sarah Maness, PhD, MPH, Department of Health Education and Promotion at East Carolina University, for additional editorial assistance and review.
The Institutional Review Board at East Carolina University has reviewed all data collection protocols utilized for purposes of this article and provided IRB approval (IRB: UMCIRB 25-001825). All data presented were fully de-identified prior to investigator access.
Financial support
The Healthier Lives at School and Beyond Telemedicine Program has received generous funding from the following sources: Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (DHHS) Office for Advancement of Telehealth; Anonymous Trust; The Harold H. Bate Foundation; Foundation for Health Leadership and Innovation; United Healthcare; North Carolina Department of Health and Human Services (NCDHHS); ECU Health Foundation; and North Carolina Blue Cross Blue Shield.
Disclosure of interests
The author and program affiliates have no relevant disclosures to report.
Correspondence
Address correspondence to Erika Taylor, 101 Heart Dr. Mail Stop 654 Greenville, NC 27834 (taylorer17@ecu.edu).
