Introduction
Youth mental health is an urgent public health concern in North Carolina. Suicide is the second leading cause of death among youth aged 10–18 in the state, underscoring the need for stronger prevention and early intervention systems.1 Surveillance data further illustrate the scope of the problem. The 2023 North Carolina Youth Risk Behavior Survey (YRBS) found that 18% of high school students reported seriously considering attempting suicide, 9.5% reported attempting suicide, and 39% reported persistent feelings of sadness or hopelessness during the previous year.2 These indicators highlight the need for systems that promote mental health literacy, identify students at risk, and connect youth and families to appropriate behavioral health services to address the promotion of mental health and well-being and the prevention and treatment of mental and substance use disorders.3
Schools are becoming critical access points for youth mental health services. As universal institutions serving nearly all children, schools provide consistent opportunities for prevention, early identification, and connection to care. National estimates indicate that almost one half of schools provide mental health services,4 and schools are the most common location of care for youth with symptoms.5 Recognizing the unique role schools can play in expanding access to care, North Carolina launched Project AWARE (Advancing Wellness and Resiliency in Education), locally branded as NC ACTIVATE (Advancing Coordinated and Timely Interventions, Awareness, Training, and Education)—referred to here as NC AWARE—in 2018. Implemented through collaboration between the North Carolina Department of Public Instruction (DPI) and the North Carolina Department of Health and Human Services (NCDHHS) and funded by the Substance Abuse and Mental Health Services Administration (SAMHSA) State Education Agency grant program, NC AWARE was designed to strengthen comprehensive school mental health systems through coordinated prevention, early identification, and expanded access to behavioral health services within school communities.
School-Based Behavioral Health Infrastructure
School-based behavioral health infrastructure plays a critical role in supporting student well-being from early childhood through adolescence. Effective school-based systems promote coordinated care through collaboration among educators, school support professionals, families, and external health and community partners. Partnerships with health organizations, behavioral health providers, and local agencies help ensure that students receive timely and appropriate services. Organizational alignment among participating stakeholders, including students, families, administrators, teachers, Specialized Instructional Support Personnel, health systems, and community agencies, is a key component of sustainable school mental health systems.
The Multi-Tiered System of Supports (MTSS) Framework
In NC AWARE, participating districts strengthened school-based mental health infrastructure to support the full continuum of services students may require. The initiative promotes a multi-tiered system of supports (MTSS) framework that integrates universal promotion and prevention, screening, targeted interventions, intensive services, and family and community engagement. Also applied to students’ academic supports, MTSS is a promising approach to address a continuum of services for students’ well-being, from universal programs to more targeted and intensive services that provide specific evidence-based interventions in small group or individual settings.6,7 Recognizing the interrelatedness of academic performance and student well-being, NC AWARE embeds mental health services within existing school systems rather than layering parallel structures.
Tier One. Universal (core) supports focus on promotion and prevention for all students and are delivered schoolwide. Examples include social-emotional learning curricula, bullying prevention programs, mental health literacy education, and wellness promotion. Schools may also implement school climate strategies such as Positive Behavioral Interventions and Supports (PBIS), trauma-informed practices, restorative discipline approaches, and universal mental health screening.
Tier Two. Targeted supports provide supplemental assistance for students requiring additional help beyond universal strategies. These services may include small-group counseling, targeted social skills instruction, and coordinated referral and progress monitoring processes.
Tier Three. Intensive supports provide individualized services for students with significant mental health needs. These supports may include individual counseling, crisis intervention, wraparound services, and individualized support teams that coordinate care across school, family, and community providers.
Within NC AWARE, districts implemented this framework by expanding educator training, strengthening referral pathways to community behavioral health providers, and increasing access to school-based behavioral health services. Because many mental health conditions emerge during childhood and adolescence, strengthening youth mental health infrastructure has the potential to influence population health outcomes across the lifespan, including educational attainment, workforce participation, and overall health status.8,9
Funding Context
SAMHSA awards Project AWARE State Education Agency grants in five-year cohorts. These grants support capacity building at both the state and local levels to advance wellness and resilience in educational settings through awareness, training, and services.10 North Carolina has received two grants through which six Local Education Agencies (LEAs) served as pilot transformation zones to develop scalable models for sustainable school-based mental health systems. Cohort 1 (2018–2023) provided grant funding for project implementation in Beaufort County, Cleveland County, and Rockingham County. Cohort 2 (2021–2026) supported Project AWARE implementation in Jackson County, Nash County, and Sampson County (Appendix A contains more details about grant funding and award amounts).
Program Design
NC AWARE promotes innovative service delivery consistent with recommendations from the NC School Mental Health Initiative. The initiative emphasizes: 1) the development of a continuum of supports and services; 2) strategies to foster sustainability, and 3) engagement of families, schools, and community partners.
Each participating Local Education Agency (LEA) provides a menu of services and evidence-based practices to address students’ mental health through the MTSS framework. NC AWARE established four primary goals:
-
Improve behavioral and psychological indices of school engagement and decrease disciplinary events through universal prevention within MTSS.
-
Reduce dropout rates, suicide attempts, and substance use by increasing access to supplemental and intensive services.
-
Improve coordination and sustainability through increased family and community engagement.
-
Increase the knowledge and effective practice of school staff in recognizing and responding to student mental health needs.
Each LEA had discretion in the practices implemented to accomplish each of these goals. Research notes that a program’s adaptability to fit the local context affects its success,11 and NC AWARE supports local programmatic decisions and the selection of evidence-based practices tailored to the specific needs of each LEA. In addition, DPI and NCDHHS provide opportunities for cross-collaboration across districts through regional school mental health teams, state mental health implementation partners, DPI’s Integrated Academic and Behavior Systems team (social and emotional learning [SEL] partners), and monthly collaboration meetings. Finally, DPI and NCDHHS provide an implementation framework that outlines a quarterly stepwise structure for key components required for successful implementation. These components include recommendations around evidence-based practice selection, universal screening, coaching, and fidelity review. Appendix B contains a detailed discussion of program evaluation and data collection, and limitations on evaluation findings.
Policy Implementation
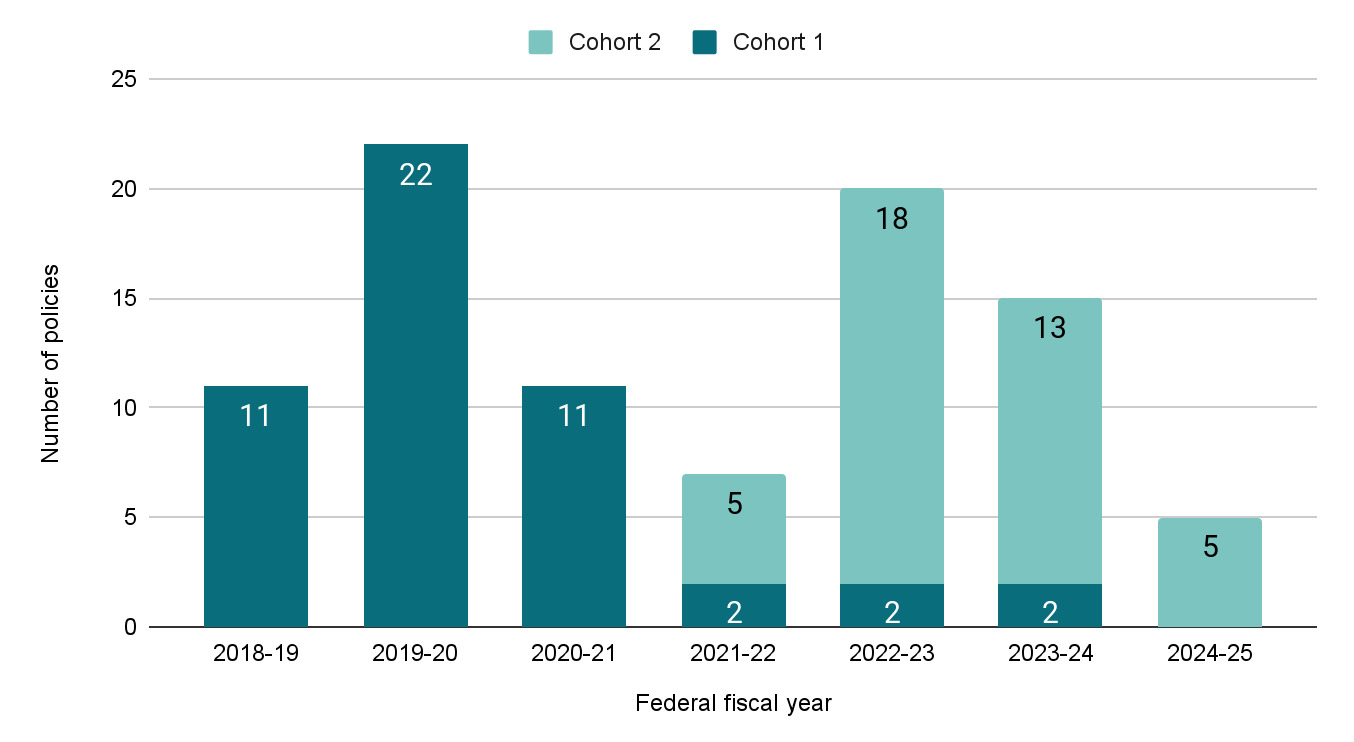
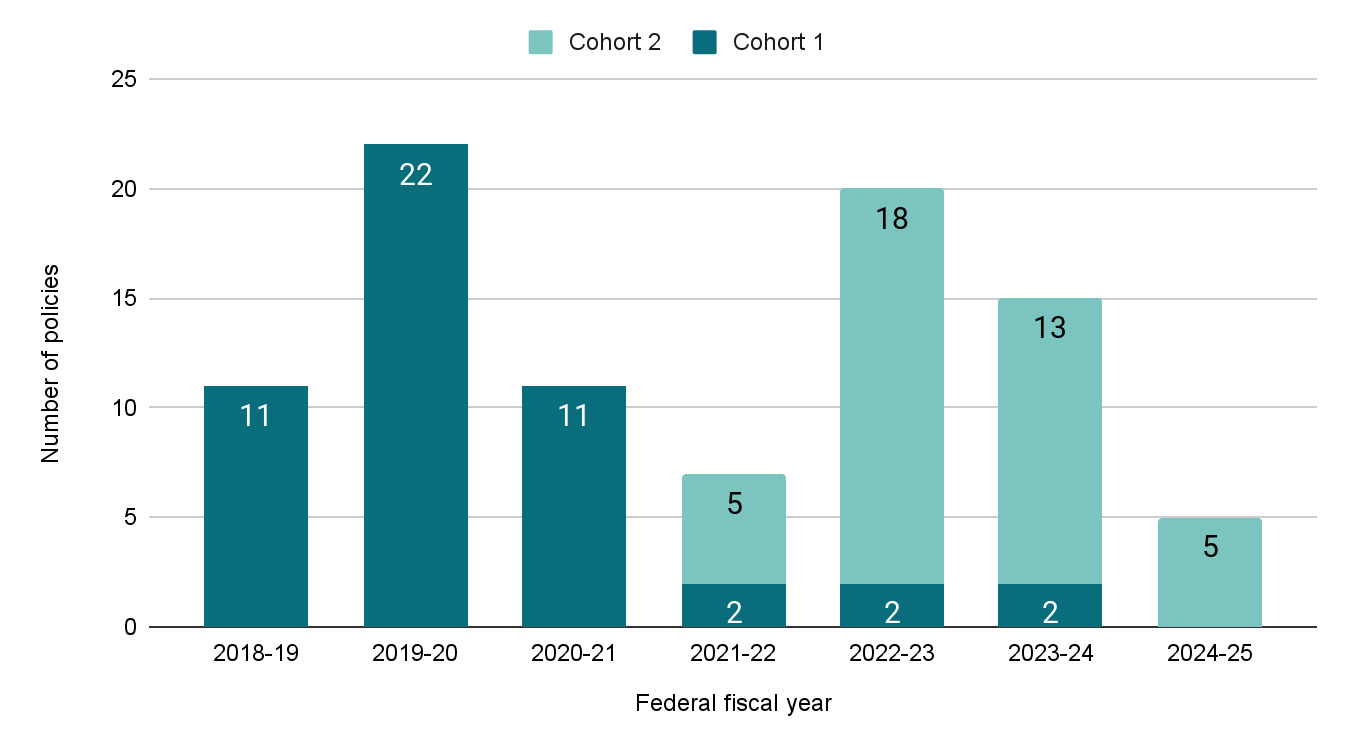
Policies and procedures that integrate mental health approaches into daily activities and school processes facilitate implementation and provide infrastructure.12,13 Together, NC AWARE LEAs implemented or amended over 90 policies to support long-term sustainability of grant activities. Implementation planning emphasized the creation of local policies at grant initiation to provide protocols and processes for referral systems, screening approaches, disciplinary action, and data collection.
Across both cohorts, the majority of policies addressed mental health referral systems, including the use of evidence-based practices in the clinical setting, admission criteria, mechanisms for clinician oversight, policies for limiting student time out of class, and parental consent for services. LEAs in Cohort 1 placed additional focus on the creation and improvement of risk assessment and suicide ideation protocols, with 12 such policies created or amended over the course of the grant. Following the creation of NC AWARE’s Suicide Risk Protocol, 69 of 115 public school units in North Carolina used this protocol as part of their School Mental Health Plan submission in 2021. In Cohort 2, policies also address approaches to Medicaid reimbursement, including enrollment, parental consent, and mental health team procedures when seeking reimbursement. Figure 1 shows the number of policies implemented in each of the cohorts by year.
Workforce Development and Evidence-Based Practices
Providing training in evidence-based practices is a key component of NC AWARE. By grounding interventions in research-proven strategies, the grant ensured that its initiatives were not only innovative, but also effective. LEAs implemented practices through smaller pilot programs and comprehensive training, aiming to equip educators with the necessary skills to address the needs of their school community. Then, they expanded selected practices district-wide. Combined, the three LEAs in Cohort 1 offered 26 different evidence-based practices, and the LEAs in Cohort 2 offered 10 different practices. In total, NC AWARE LEAs reported almost 54,000 training participants since 2018–2019.
LEAs in both cohorts included substance abuse education in their evidence-based practices to address students’ behavioral health and provide disciplinary alternatives to drug-related infractions. Each LEA found different practices most effective for their district and sometimes for different student populations and ages. Broadly, NC AWARE LEA leaders recommend a comprehensive approach that includes practices that address all three levels of MTSS intervention. In addition, NC AWARE leaders found that providing the district with a comprehensive list of available evidence-based practices and relevant resources and lesson plans by student age through a shared folder encouraged fidelity.
Pilot LEAs also found success with regular (monthly) professional development opportunities for clinical staff. Over the grant period, both cohorts expanded professional development opportunities and increased staff capacity to identify and respond to student behavioral health needs, as shown in Table 1. In Cohort 2, training participants complete post-training surveys to understand whether participants gain knowledge and skills as a result of training; to date all participants indicated an increase in knowledge.
System Coordination
Districts reported improved collaboration with local community mental health providers and increased family engagement in planning and service delivery. Statewide, NC AWARE built coordinated care networks through the creation of almost 50 partnerships. Agreements emphasized relationships that would build clinical staffing support within the district through local Managed Care Organizations, mental health providers, external funding providers, and local universities. The most recent partnerships in NC AWARE emphasize clinical care for students and supporting licensure and continuing education for clinicians working in the schools. Local implementation fidelity monitoring through school behavioral health teams show improved integration of behavioral health supports within schools’ MTSS frameworks.
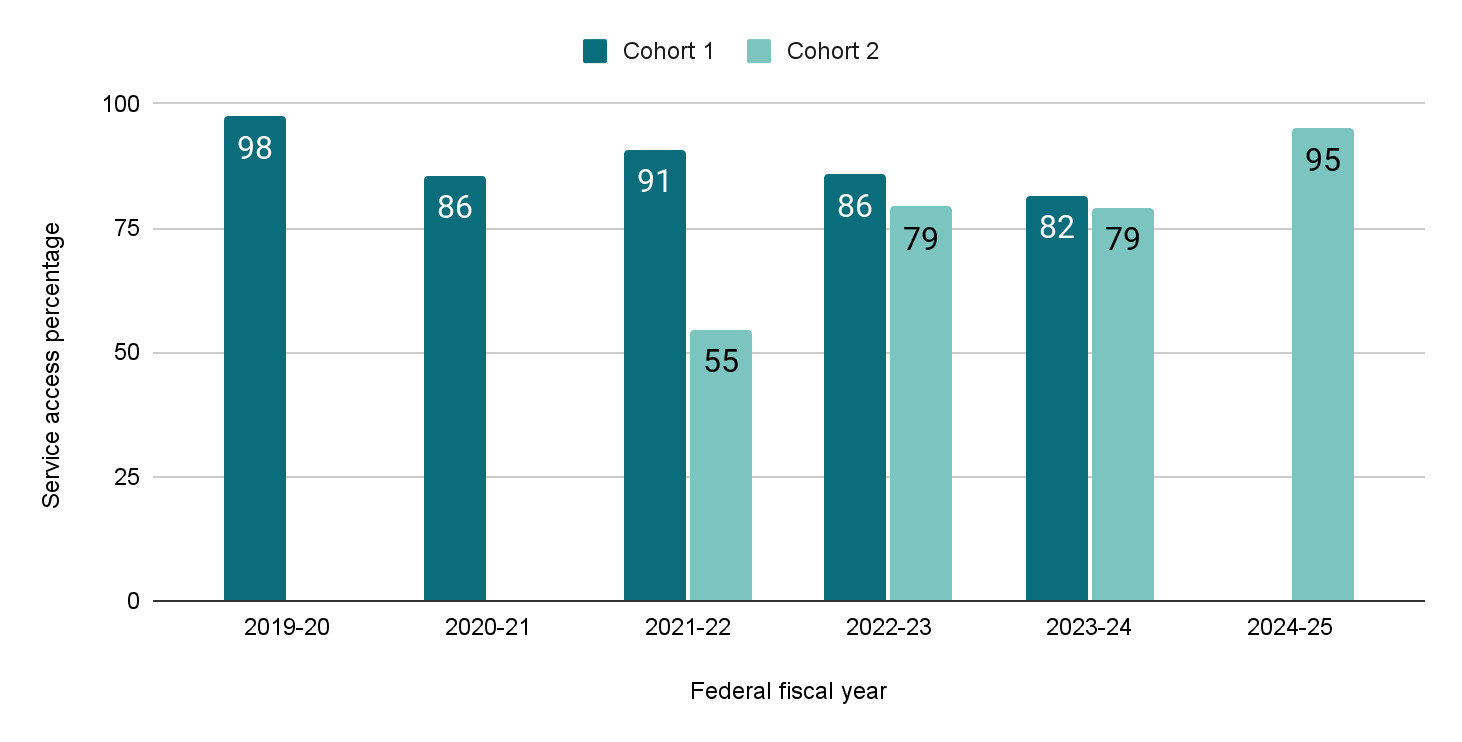
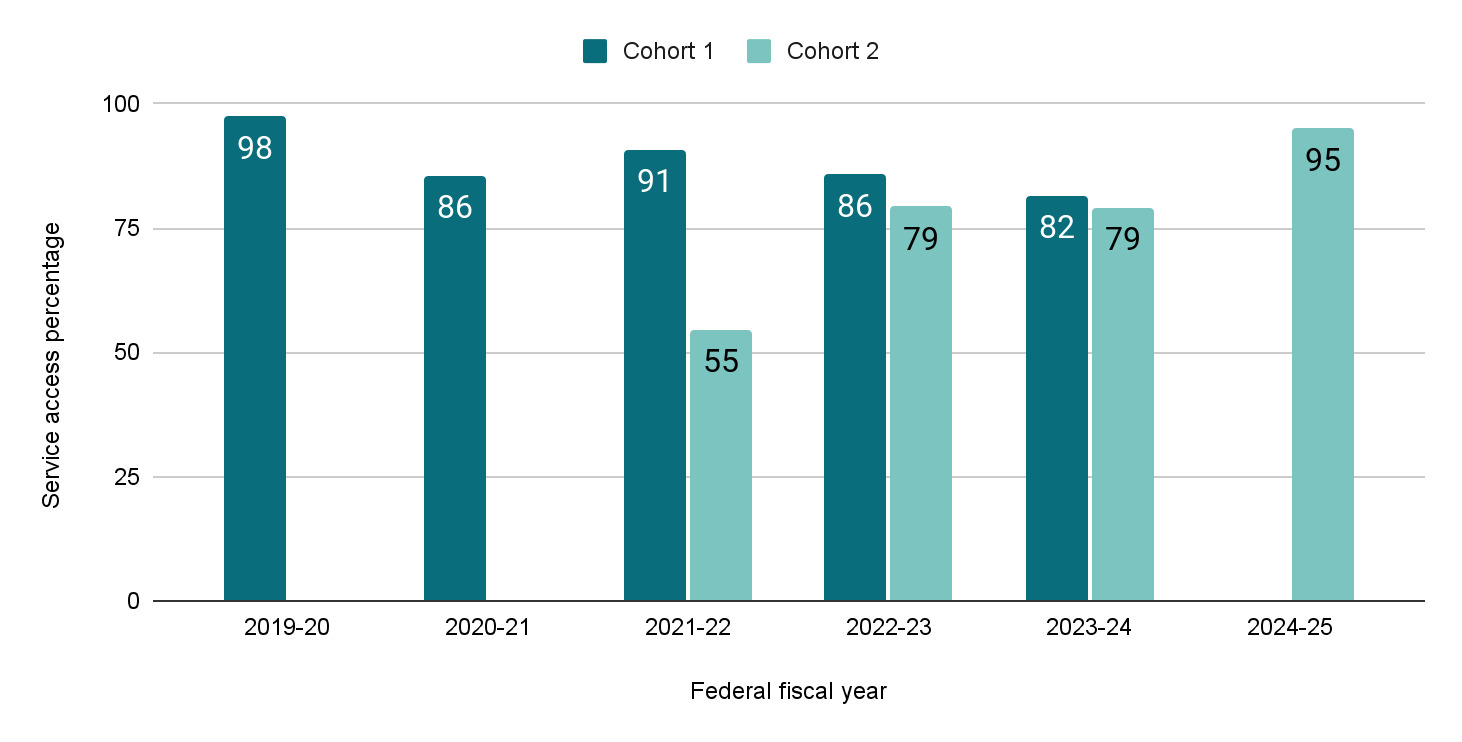
System coordination and staffing resulted in an average of almost 4000 students served each year through NC AWARE since 2019. Cohort 1 showed an average access rate (percent of students who receive services out of total referred) of 89%; the current average in Cohort 2 is 77%. In addition, Cohort 2 shows annual increases in access rates since implementation began (Figure 2).
Long-Term Outcomes
In line with grant goals to improve student engagement, NC AWARE considers several long-term outcomes at the district level: student attendance, student dropout rates, and discipline rates. Throughout the grant, providing these services to students was expected to result in overall district improvement regarding the outcomes. Trends in district-level outcomes are uneven across cohorts and districts. The NC AWARE team is exploring options to track individual long-term outcomes among students who receive services, which would provide a more proximate measure of program implementation. Preliminary analyses demonstrate LEA-specific reductions in selected outcomes, including:
-
Reduced annual dropout rates among Cohort 1 LEAs between 2020–2021 and 2022–2023.
-
Increased teacher satisfaction with student conduct in the classroom among Cohort 1 LEAs between 2020 and 2024.
-
Reduced in-school suspension rate per 1000 students for Samson County between 2022–2023 and 2023–2024.
-
Reduced in-school suspension rate per 1000 students for Jackson County between 2023–2024 and 2024–2025.
-
Reduced rates of chronic absenteeism among Cohort 2 districts since 2020–2021 and 2023–2024.
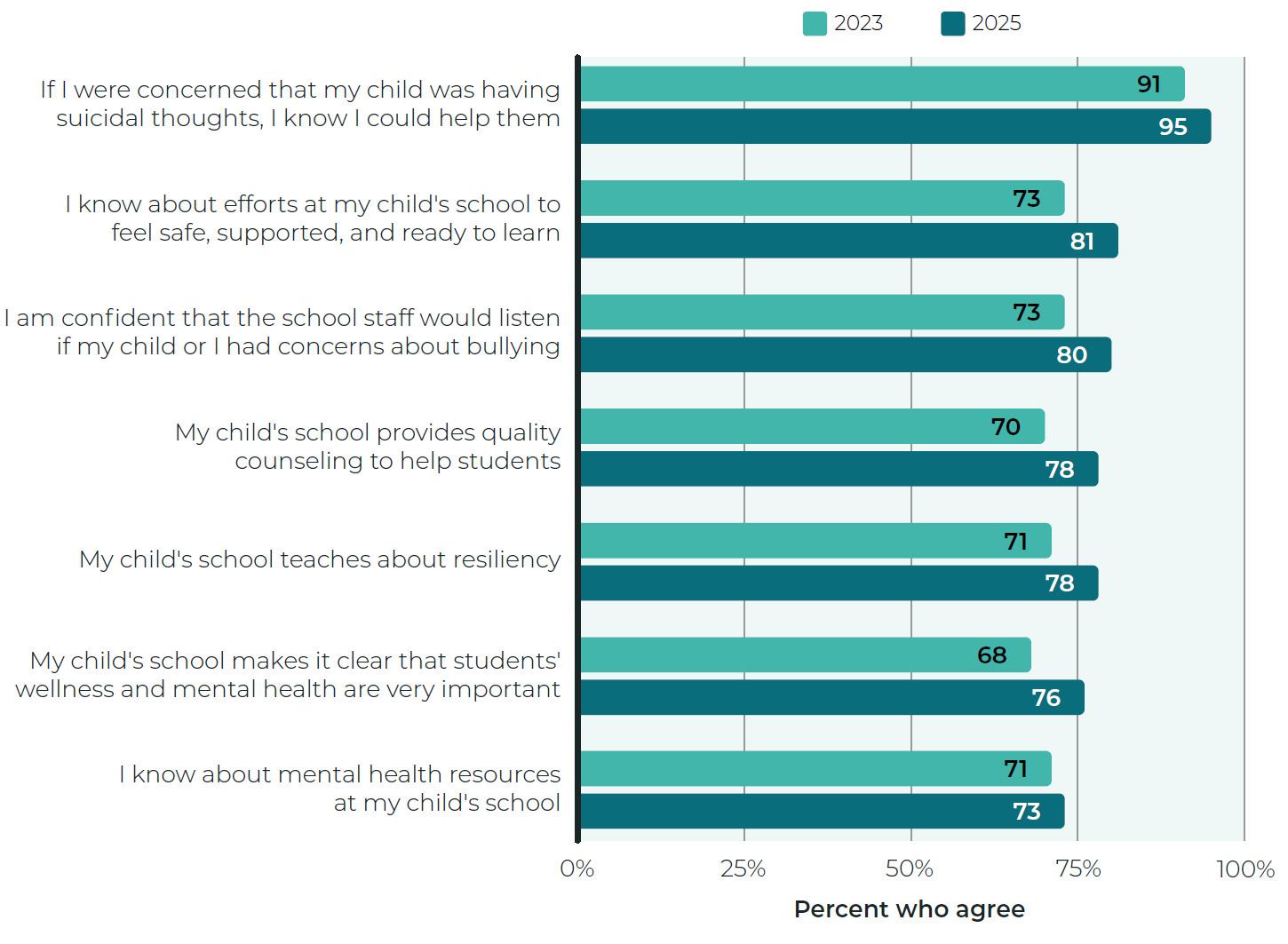
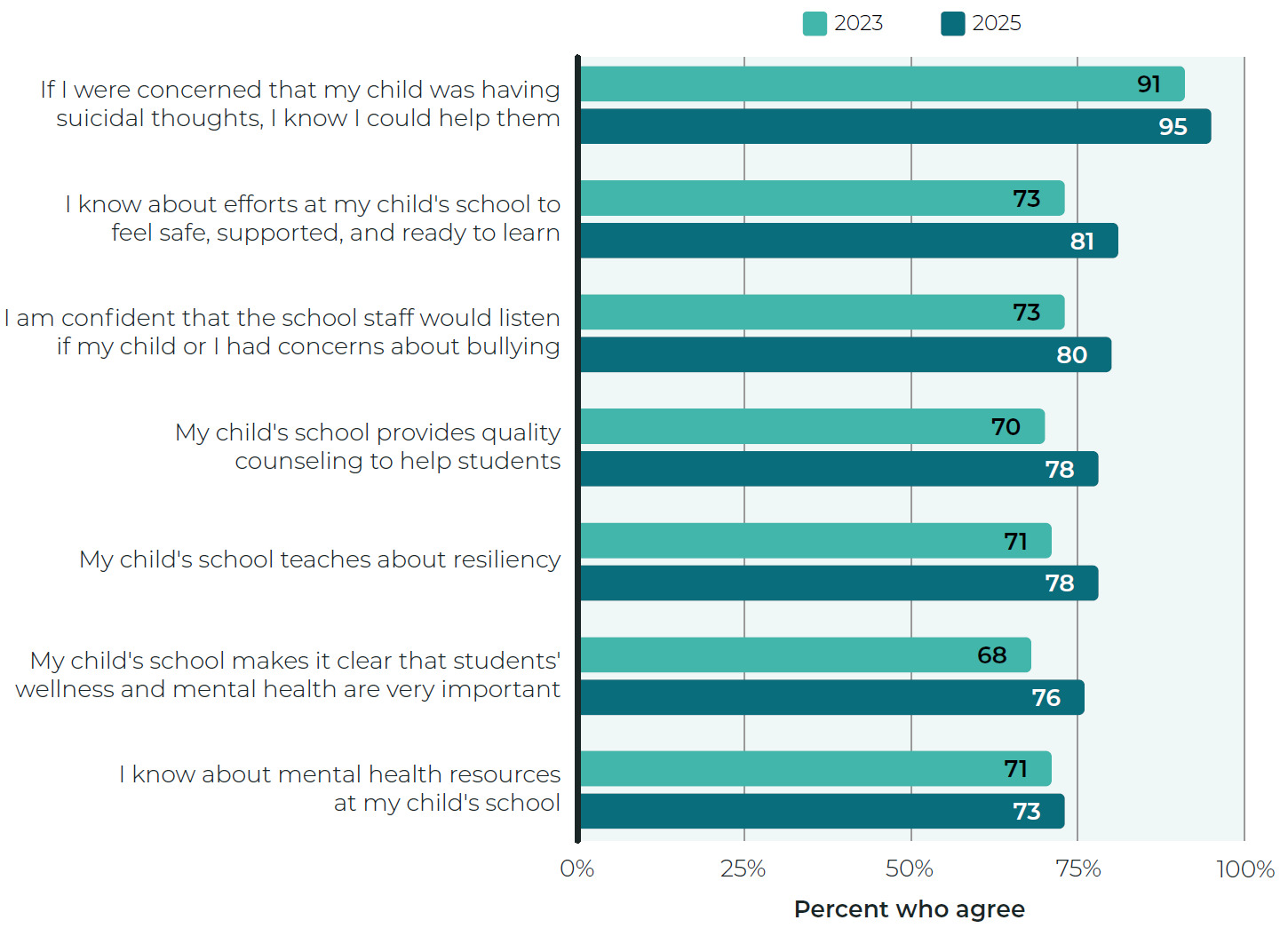
One area of significant growth for Cohort 2 is in LEA engagement with families. Families in each district were surveyed at two points in time (year two and year four of the grant). Compared to 2023, families in 2025 showed increased awareness of district mental health services across all three districts. In particular, family perceptions of school focus on students’ mental health, efforts to make students feel safe and supported, and the provision of quality counseling increased eight percentage points over two years. Figure 3 provides an overview of family responses across all three sites in 2023 and 2025. In addition to these measures, families also reported increased collaboration on children’ s mental health services and increased willingness to seek help for a child’s mental health if the child showed changes in thinking, feeling, or behaving.
Next Steps
Sustainability and Medicaid Alignment
While grant funding supported the initial development of school mental health systems, long-term sustainability requires stable and scalable financing mechanisms. To support this transition, NC AWARE partnered with the Rural Opportunity Institute, a North Carolina-based nonprofit organization, to establish a Medicaid Learning Collaborative designed to assist LEAs in implementing school-based Medicaid billing. The collaborative provides structured technical assistance, individualized coaching, and peer learning opportunities to strengthen district capacity for Medicaid reimbursement. Through this approach, participating districts are supported in developing billing infrastructure, strengthening cross-sector coordination, and integrating Medicaid as a sustainable financing strategy for school-based behavioral health services.
Early findings from the collaborative indicate improved district understanding of Medicaid policies and billing processes, as well as increased planning for long-term sustainability of school-based mental health services. Efforts to align school mental health services with Medicaid financing may offer an important pathway for expanding access to care and sustaining school-based behavioral health systems beyond the life of grant funding.
Benefit-Cost Analysis
Despite promising implementation and early outcome data, long-term funding for expansion and sustainability is not guaranteed. To better inform future investment decisions, a comprehensive benefit–cost analysis (BCA) led by the UNC Collaboratory is underway. A more detailed discussion of the benefit-cost analysis can be found in Appendix C.
Conclusion
Youth mental health challenges continue to affect the well-being and long-term outcomes of students across North Carolina. Schools play a critical role in early identification and connection to behavioral health services, positioning them as key partners in expanding access to care. NC AWARE demonstrates how cross-agency collaboration can strengthen school-based mental health infrastructure by integrating prevention, early identification, and coordinated care within educational settings. Through implementation of MTSS, external evaluation, and sustainability planning, North Carolina has begun to transition from pilot initiatives to scalable statewide infrastructure. Continued investment in workforce development, system integration, and sustainable financing mechanisms—including Medicaid alignment—will be essential to sustaining and expanding school-based mental health services and improving long-term population health outcomes for North Carolina’s youth.
Author Contributions
Austin and Warner-Griffin jointly conceptualized the manuscript. Austin led statewide implementation and contributed programmatic expertise. Warner-Griffin led evaluation design and data analysis. Both authors contributed to the interpretation of findings, manuscript drafting, and final revisions.
Financial support
This work was supported by Project AWARE funding through the Substance Abuse and Mental Health Services Administration.
Conflicts of Interest
The authors report no conflicts of interest.
Correspondence:
Address correspondence to Dr. Heidi E. Austin, North Carolina Department of Public Instruction, Raleigh, NC (heidi.austin@dpi.nc.gov).