
North Carolina’s behavioral health crisis system faces a structural capacity problem. Despite investments in mobile crisis teams, Facility-Based Crisis Centers (FBCCs), and the 988 Suicide & Crisis Lifeline, access is still uneven across North Carolina. As a result, emergency departments (EDs) function as a primary psychiatric safety net. This produces prolonged psychiatric boarding, delayed initiation of psychiatric pharmacologic treatment, increased health care expenditures, and worsening patient outcomes.1 In North Carolina this is not just a service gap, it’s a measurable workforce and infrastructure failure requiring extensive policy reform.
Psychiatric boarding refers to the practice of holding a patient in an ED after a decision has been made to admit them, due to a lack of available inpatient psychiatric beds. For example, a patient who presents after a suicide attempt may be medically stabilized within a few hours but then stay in the ED for 24–72 hours waiting for psychiatric placement. During this time, these patients are under continuous observation but are without access to structured therapy or appropriate medication optimization; care is also largely supervisory rather than therapeutic, consisting of safety monitoring and reassessment rather than active psychiatric stabilization.
Psychiatric patients often experience significantly longer boarding times than medical patients.2 Nationally, boarding frequently exceeds 24 hours and can last several days.2 These patients often present with conditions requiring inpatient psychiatric admission, including active suicidal ideation or suicide attempts, acute psychosis, severe mood disorders, bipolar disorder with mania or agitation, and substance-induced psychiatric crises. Psychiatric patients account for approximately 21.5% of all ED boarding cases and remain boarded nearly three times longer than medical patients.2
In North Carolina, limited inpatient psychiatric bed capacity and geographic gaps in crisis centers contribute to this problem. Psychiatric boarders prevent an average of 2.2 potential ED bed turnovers per patient, representing an estimated $2,250 in lost revenue per occupied bed.2 From the perspective of the State, this is both a public health and systems efficiency issue.1 This prolonged use of ED space shows how psychiatric boarding is not just a delay in care, but a costly misdistribution of health care resources.
From 2006 to 2014, emergency department visits for suicidal ideation increased by 414.6%, reflecting an increase in acute psychiatric presentations without a corresponding expansion of inpatient or crisis capacity.2 National trends show that psychiatric bed supply has remained the same or declined over time, even as mental health demand has increased.3 This rise in acute psychiatric patient presentations places pressure on EDs to absorb patients who would otherwise be managed in specialized psychiatric settings. As demand increases without enough growth in inpatient beds or workforce capacity, more patients are held in the ED for extended periods. The discrepancy between rising psychiatric demand and limited capacity shows a cycle of delayed treatment, increased ED usage, and higher health care costs.
However, the problem extends beyond gaps in system design. According to US Health Resources and Services Administration (HRSA) data, North Carolina currently has 229 designated Mental Health Professional Shortage Areas (HPSAs).4 These shortages extend across facility, geographic, and population-based designations throughout the state, demonstrating that workforce gaps are not isolated but widespread across multiple counties. Figure 1 shows that the majority of these HPSAs fall within the high severity range, reinforcing that these are not minor shortages but deep-seated workforce deficits.

The severity of these shortages warrants a major concern. Approximately 80% of HPSAs (181 of 229) fall within the high-severity category (14–25 on a 26-point scale).4 This indicates that most of North Carolina’s shortage areas are not marginally underserved; they represent high-need, structurally deficient workforce regions.4 High-severity HPSA designations reflect areas where provider-to-population ratios are critically low, often resulting in long wait times for psychiatric care, limited availability of outpatient services, and reduced access to crisis intervention resources. At this scale, workforce shortages go beyond limiting routine care; they delay treatment, worsen psychiatric conditions, and increase ED reliance.
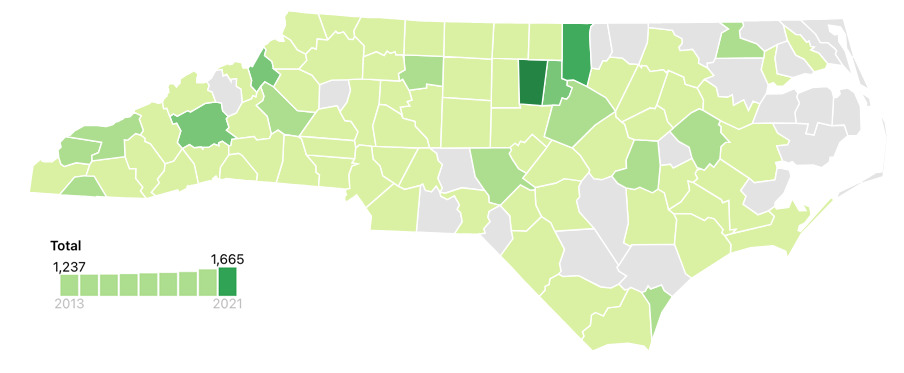
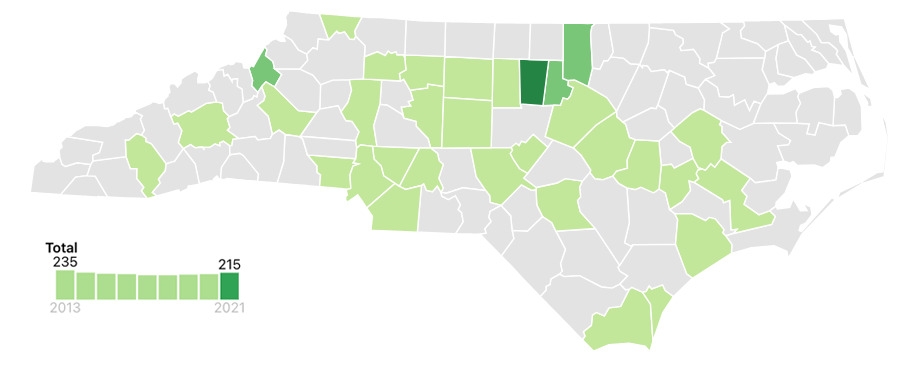
Workforce data from the UNC Cecil G. Sheps Center for Health Services Research further shows the distribution problem. Although the total number of psychiatrists in North Carolina increased from 1237 psychiatrists in 2013 to 1665 psychiatrists in 2021, this growth has been concentrated in urban counties (e.g., Wake, Durham, Mecklenburg), with limited or no psychiatric coverage in rural regions (Figure 2).4,5 The pediatric psychiatric workforce is even more concerning. The number of child and adolescent psychiatrists declined from 235 in 2013 to 215 in 2021.4,5 Numerous counties have no child psychiatrists, as shown in Figure 3.
.png)
.png)
EDs are not designed to provide extended psychiatric stabilization.1 Boarding delays initiation of antipsychotics or mood stabilizers, which can increase risk of self-harm, aggression, and long-term destabilization.1,2 Delayed stabilization is associated with worse clinical outcomes and increases likelihood of repeat ED visits.2,6 In addition to patient harm, prolonged ED boarding contributes to hospital overcrowding and clinician burnout.
Crisis stabilization services are significantly less costly than inpatient or ED care and are clinically appropriate for many psychiatric emergencies.7 As patients move upward toward inpatient or long-stay facilities, costs increase substantially. When outpatient crisis services are lacking, patients are forced into higher-cost settings. This increases total system expenses. When these services are unavailable, the state pays more for lower-value, lower-quality care. With approximately 80% of mental health HPSAs classified as high severity, North Carolina faces a structural provider problem that can’t be resolved through minor adjustments.7 In 2023, the North Carolina General Assembly allocated nearly $230 million toward behavioral health system transformation, including expansion of crisis stabilization centers and mobile response teams.8 However, this investment is insufficient relative to the scale of need, and gaps in lower-cost crisis services shift patients into higher cost settings, leading to a less efficient system and increased health care spending.
North Carolina has made some investments:
-
Launch of 988 Suicide & Crisis Lifeline (2022).7,9,10
-
Expansion of mobile crisis teams.7,9,10
-
Development of Facility-Based Crisis Centers.7,9,10
-
Medicaid expansion (2023), increasing behavioral health coverage eligibility.1,8
Despite these investments, the state continues to face funding instability and reductions in psychiatric bed capacity, reflected in persistent delays for inpatient placement and prolonged ED boarding times. As a result, limited bed availability continues to drive longer ED stays and increased health care costs, highlighting the need for long-term, sustainable reform.2,8 However, major challenges remain:
-
Crisis centers are not located in every county.
-
Inpatient psychiatric beds remain limited.
-
Workforce shortages persist, especially in rural areas.
-
Coordination across LME/MCO regions varies.
Inpatient psychiatric bed capacity remains a critical constraint. National estimates suggest approximately 18 beds per 100,000 population, which is well below the recommended benchmark of 40-60 beds per 100,000.11,12 North Carolina faces even greater limitations, with publicly funded state psychiatric bed availability estimated at approximately 4.2 beds per 100,000 population.13 Even the minimum threshold for adequate capacity, estimated at approximately 30 beds per 100,000 people, is not met, demonstrating that both national- and state-level capacity fall far below minimum standards for proper psychiatric care.12
The result is a “Band-Aid” system in which geography determines access. To address this issue, North Carolina has several potential policy pathways:
-
Status quo: minimal improvement, no structural change, continued high costs.
-
Targeted expansion: partial relief, moderate ED reduction, workforce limited.
-
Comprehensive reform: structural change, significant ED reduction, upfront cost with long-term savings.
The first option is to maintain current infrastructure with steady growth. This approach would rely primarily on Medicaid expansion and existing Managed Care contracts to gradually increase crisis capacity.8 While politically feasible, this approach doesn’t address the fact that 80% of mental health HPSAs are high severity. Limitations include slow growth, continued rural disparities, and persistent ED boarding.
The second option is targeted infrastructure expansion. This means that North Carolina would prioritize state-funded expansion of crisis stabilization centers in high-HPSA counties. Advantages include reduced ED utilization, improved geographic equity, and provision of lower-cost stabilization settings. However, this approach remains dependent on workforce availability. Infrastructure without workforce expansion won’t solve the underlying problem.
The third option is comprehensive crisis reform. This means North Carolina would try to adopt a coordinated statewide crisis model similar to other states. An example of a model to follow would be Arizona’s “Crisis Now” framework, which uses hotline triage, mobile response, crisis stabilization units, and real-time bed tracking.14 The North Carolina version for implementation of the crisis model would be completed by legislative funding for crisis infrastructure, a statewide psychiatric bed tracking system, telepsychiatry in rural hospitals, workforce loan repayment, and recruitment incentives. SAMHSA’s national crisis care guidelines emphasize the “someone to call, someone to respond, and somewhere to go” framework, which has been associated with reduced emergency department utilization when implemented fully.7 Delays in psychiatric treatment are associated with worse outcomes, as demonstrated in early coordinated care models such as the NIMH RAISE program.6 One national analysis found that 65% of psychiatric patients who boarded in the ED experienced at least one medication error, with 89% of those errors involving omission of home psychiatric medications.2 This highlights that psychiatric boarding is not simply a delay in care but may disrupt continuity of treatment and increase the risk of clinical deterioration.
North Carolina’s best approach would be to pursue comprehensive crisis continuum reform rather than incremental expansion. Incremental reforms are unlikely to reduce ED boarding or correct disparities in rural communities. The General Assembly should:
-
Establish dedicated crisis funding separate from Managed Care contracts.
-
Expand workforce loan repayment programs that focus on psychiatric providers.
-
Implement a real-time psychiatric bed tracking system.
-
Invest in telepsychiatry to help support rural EDs.
To make this approach operational, funding considerations need to be addressed. While comprehensive crisis reform requires upfront investment, existing data demonstrate that crisis stabilization services offer a more cost-effective alternative to current system inefficiencies. Crisis stabilization services have been estimated to cost approximately $1,085 per patient, with studies demonstrating a return of $2.16 for every $1.00 invested.15 In contrast, psychiatric boarding in emergency departments may cost approximately $2,700 per day, reflecting a substantial financial burden associated with delayed placement and inefficient care delivery.16
State-level reimbursement data further shows that crisis intervention services are often funded at several hundred dollars per day, reinforcing their role as a lower-cost alternative to inpatient psychiatric hospitalization.15,17 National analyses also indicate that behavioral health crisis services are associated with reduced emergency department utilization and improved system efficiency.18 Given that emergency department care remains a high-cost setting for behavioral health treatment, the North Carolina General Assembly could pursue funding through a combination of Medicaid-supported services, federal matching opportunities, and reallocation of expenditures from inefficient emergency care utilization.19 Importantly, national analyses suggest that underinvestment in psychiatric care shifts care toward higher-cost emergency settings.3,18
While this approach requires significant upfront investment, it is likely to produce downstream savings by producing reductions in avoidable ED utilization and inpatient admissions. Crisis stabilization services are lower cost than inpatient hospitalization and improve clinical outcomes when implemented effectively.4 Continued reliance on ED boarding, by contrast, increases Medicaid expenditures, strains hospital systems, and leaves vulnerable patients in prolonged, non-therapeutic environments where their conditions may worsen without timely psychiatric intervention.
Conclusion
Taken together, these findings highlight that North Carolina’s current mental health crisis system, while improved in recent years, remains uneven and insufficient. The continued reliance on EDs for psychiatric crisis delays treatment, increases system costs, and worsens patient outcomes. From a Managed Care perspective, this represents a misallocation of resources: high-cost emergency settings are being used for conditions that could be managed more effectively in specialized crisis environments. A comprehensive, coordinated crisis continuum model—supported by legislative funding, workforce investment, and telepsychiatry integration—offers the strongest pathway toward improved patient outcomes, reduced ED boarding, and long-term cost containment. Without structural reform, emergency departments will continue functioning as the state’s primary psychiatric safety net, an arrangement that is clinically suboptimal and fiscally inefficient.
Acknowledgments
The author thanks Professor Jon Easter, BSPharm, RPh; Julianna Mercado, Doctor of Pharmacy Candidate at the UNC Eshelman School of Pharmacy; and reviewers who provided valuable feedback and support during the development of this work.
Financial support
None declared.
Conflicts of interest
None declared.
Correspondence
Address correspondence to Paul Alebrande, 301 Pharmacy Lane, Chapel Hill, North Carolina 27599 (pale@unc.edu).