Background: What is the Care Management for High-Risk Pregnancy Program and What Makes It Work?
The Care Management for High-Risk Pregnancy Program (CMHRP) is North Carolina’s core vehicle for delivering care management to pregnant Medicaid beneficiaries at risk for adverse birth outcomes. CMHRP has historically been delivered through local health departments (LHDs) in close partnership with prenatal care providers.1–3 The program’s logic is straightforward: identify risk early using standardized screening, then provide sustained care management to address clinical needs and social drivers of health that complicate pregnancy.4,5
This design is embedded in North Carolina’s Pregnancy Medical Home (PMH) model. PMH is a statewide enhanced prenatal care model launched in 2010 through a contract with Community Care of North Carolina (CCNC), supported by a per-member-per-month (PMPM) payment to provide care management through LHDs in collaboration with PMH providers.5 Participating PMH providers agree to complete a standardized risk screening at the first prenatal appointment and refer patients to LHDs for case management, integrating care plans with local pregnancy care management programs and translating risk identification into relationship-centered engagement with frequent contact, problem-solving, and navigation of clinical and social needs that cannot be addressed in brief prenatal visits.2,5
Importantly, North Carolina built financing and accountability around these touchpoints. PMH providers receive incentive payments for completing risk screening and postpartum visits, reinforcing early identification and postpartum continuity as policy priorities.6 PMH pathways were developed to promote evidence-based practice statewide and reduce variation in conditions associated with adverse outcomes (e.g., hypertensive disorders, postpartum care).4,7
Evidence Supporting Universal Screening and Face-To-Face Care Management
Research on the PMH model demonstrates that standardized universal risk screening data can meaningfully stratify preterm birth risk, supporting standardized screening as more than a documentation requirement.8 Furthermore, Mallampati and colleagues evaluated the association between care management and neonatal outcomes within North Carolina’s Medicaid-managed PMH framework.9 They found clinically meaningful differences in outcomes for high-risk non-Hispanic Black birthing people: those receiving ≥ 5 face-to-face care management visits had lower preterm birth (16.9%) and a reduction in low birth weight (17.8%), as compared to those not receiving care management (25.9% and 26.7%, respectively).9 Similarly, emerging evidence suggests that ≥ 5 face-to-face care management was associated with a 9.8 percentage-point lower likelihood of developing preeclampsia among high-risk Medicaid enrollees.10 These findings are directly relevant for policy because they indicate that the intensity and modality of care management are consequential for neonatal and maternal outcomes.
Another study highlighted that despite broader neighborhood deprivation limiting prenatal access overall in North Carolina, non-Hispanic Black individuals in the most disadvantaged areas were more likely than their non-Hispanic White peers to receive care management at LHDs, underscoring the reach of the CMHRP program among non-Hispanic Black populations.11 These findings suggest that while deprivation remains a barrier, CMHRP has the potential to mitigate disparities in access to prenatal care.
What Changes Are Coming and Why Do They Matter Now?
Beginning January 1, 2027, North Carolina’s Medicaid care management environment enters a more formalized phase in which LHDs may terminate or transfer CMHRP services under standardized state guidance, and Prepaid Health Plans (PHPs) assume greater responsibility for ensuring continuity of care management services for eligible members.12 Under NC Medicaid’s Companion Guide for Care Management Service Termination and Transfer, LHDs that determine they can no longer continue CMHRP services must follow a defined pre-transfer process, after which payments for CMHRP services cease upon the effective date of discontinuance. While the North Carolina Department of Health and Human Services remains committed to continuity of care, exclusive contracting protections for LHDs have expired, and future participation will be voluntary with Managed Care Organizations (MCOs), locally known as Prepaid Health Plans (PHPs) or standard plans.
Importantly, these changes do not eliminate standardized pregnancy risk screening, which remains foundational to identifying high-risk pregnancies. However, they do alter who conducts screening, where screening results flow, and how consistently they trigger timely, intensive, relationship-based care management, which relies on providers getting accurate data by completing risk screening face-to-face with the beneficiary and care managers providing face-to-face care management services. Furthermore, there could be a loss of financial incentive for obstetric care providers to screen ($50.00) and conduct postpartum visits ($150.00),13 which constitute a substantial portion of Medicaid reimbursement. With such a substantial reduction in Medicaid reimbursement, providers may reduce or eliminate prenatal care services for Medicaid recipients.
Research in other states has shown that delegating risk screening to MCOs, who have an incentive to reduce the costs of care delivery, may inadvertently widen disparities. For example, a 2018 evaluation of a county-by-county implementation of the transition from fee-for-service (FFS) Medicaid to Managed Care in Texas showed that MCOs prioritized better care to Medicaid beneficiaries who have a lower risk of preterm birth and low birth weight while providing lower-quality care to higher-risk patients, predominantly non-Hispanic Black mothers. The study found that the mortality rates for children born to US-born Black mothers significantly increased (by 15%), while those for Hispanics significantly decreased (by 22%), causing the Black-Hispanic child mortality gap to grow by 69%. The Black-Hispanic low birth weight and preterm birth rate gaps also increased significantly.14
As a result, January 2027 marks a critical inflection point: without deliberate policy action to stabilize delivery arrangements and data workflows, universal risk screening may increasingly occur in a system where the downstream care management response is fragmented, delayed, or less intensive, placing at risk the very outcomes CMHRP was designed to improve, especially for those with health-related social needs. To further understand the consequences of this change, we surveyed the health departments currently implementing the CMHRP program. Forty-two (42) care managers and health directors representing 50 counties responded. Preliminary findings from the statewide CMHRP stakeholder survey demonstrate overwhelming support for the program’s effectiveness and patient-centered design, alongside clear concerns about the impending policy transition and persistent resource constraints, particularly in rural areas.
Near-universal agreement that CMHRP improves health outcomes. Nearly 100% of respondents agreed that CMHRP improves health outcomes for individuals with high-risk pregnancies, is acceptable to Medicaid clients and staff, and aligns with local health department missions, underscoring that CMHRP is a well-functioning, valued intervention rather than a program in need of replacement.
Uncertainty about the transition to greater health plan oversight. At the same time, respondents expressed growing unease about the January 2027 transition to greater health plan oversight, with only 73.8% expressing confidence in the program’s long-term sustainability, and many citing uncertainties about contracting, reimbursement, and the continuity of relationship-based care management. Concerns were most pronounced in rural and multi-county health departments, where respondents described closing obstetric facilities, limited transportation options, and insufficient community resources as compounding barriers to care. Exhibit 1 presents quotes from survey respondents that highlight these findings.
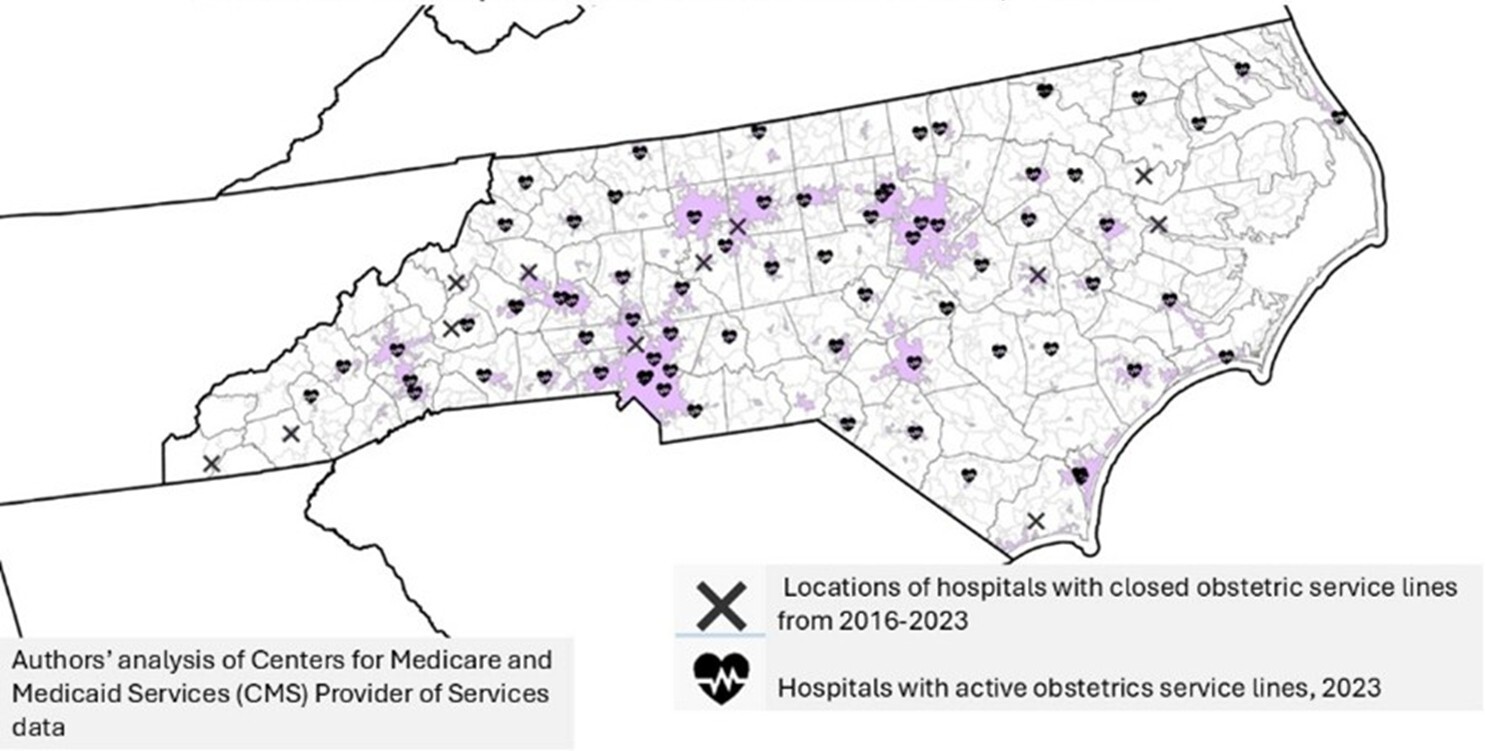
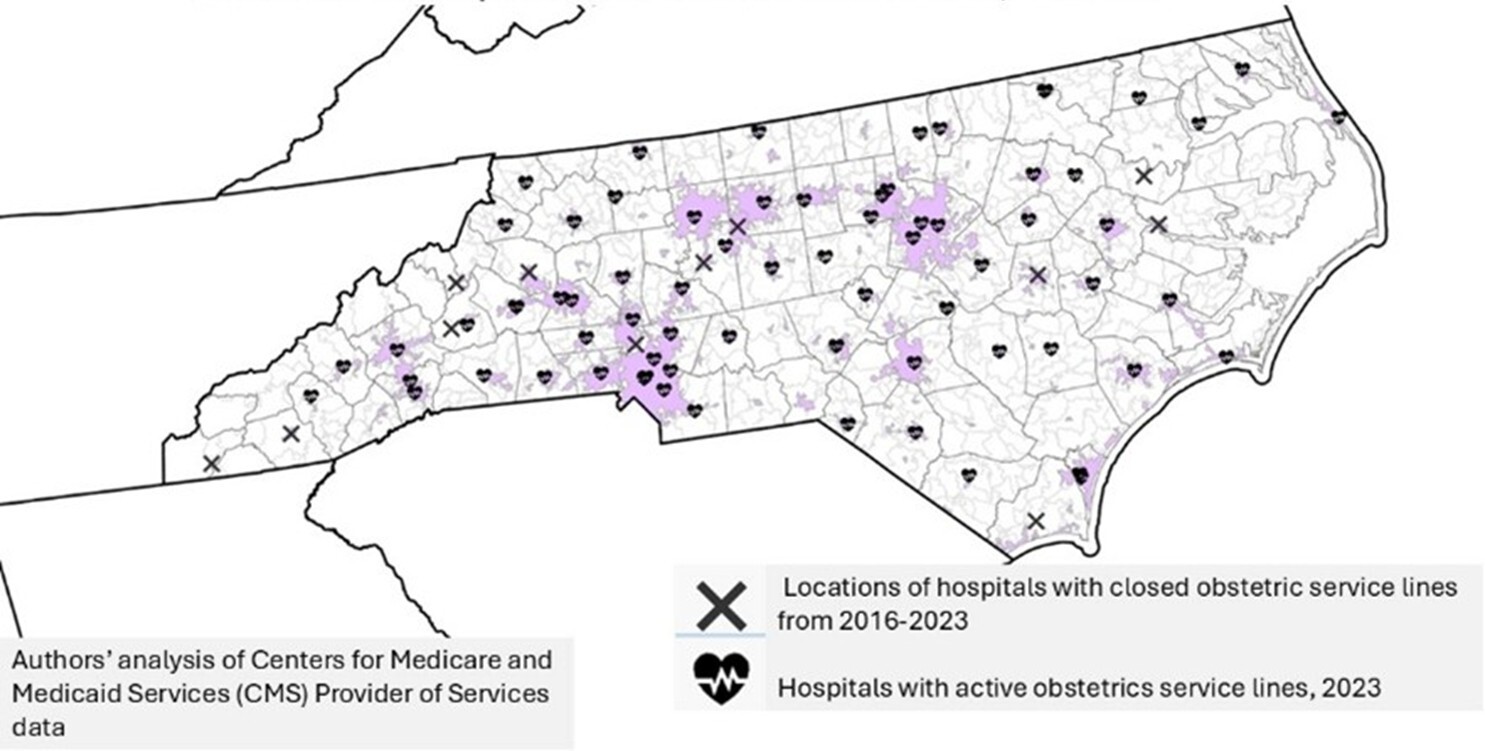
The map (Figure 1) shows widespread closure of hospital obstetric service lines across North Carolina between 2016 and 2023, with remaining OB services increasingly concentrated in metropolitan areas, leaving many rural counties with limited local delivery care. In these settings, care managers emphasized that CMHRP’s community-embedded, face-to-face model is essential for navigating structural and contextual gaps that health plans alone cannot address.
Collectively, the findings suggest that while CMHRP enjoys near-universal endorsement of its impact and implementation among frontline staff, the upcoming policy changes and unresolved inequities, especially in rural areas, pose a significant risk to the very features that make the program effective.
Implications For High-Risk Pregnancies
The findings presented in this brief have clear implications for North Carolina’s Medicaid policy as care management responsibilities evolve. First, the near-universal endorsement of CMHRP by frontline staff indicates that the program’s core design, universal risk screening paired with community-embedded care management, is working in practice. Second, the January 2027 transition introduces meaningful risk to program effectiveness if policy changes disrupt the screening-to-care-management pathway. Although standardized pregnancy risk screening will be conducted, survey respondents expressed concern that changes to contracting, referral workflows, and oversight could delay or dilute the downstream care management response. Such disruptions would undermine the very mechanism through which CMHRP achieves impact.
Third, resource constraints, especially in rural and multi-county health departments, magnify these risks. Respondents described the closure of obstetric facilities, limited transportation, delayed referrals, and insufficient community resources, all of which increase reliance on locally embedded care managers who understand the community context and can engage patients face-to-face. In these settings, shifting care management away from LHDs without adequate safeguards could exacerbate existing inequities and reduce access for those most at risk.
Key Messages
-
Care Management for High-Risk Pregnancy Program (CMHRP) is a well-functioning, evidence-supported program that effectively improves health outcomes for individuals with high-risk pregnancies by linking universal pregnancy risk screening with sustained, relationship-centered care management delivered through local health departments (LHDs).
-
The effectiveness of CMHRP depends on what happens after risk is identified, specifically, timely referral and intensive, face-to-face care management that addresses both clinical needs and social drivers of health.
-
Evidence shows that the intensity and modality of care management matter, with greater benefits observed for individuals receiving more frequent, face-to-face engagement, underscoring the value of CMHRP’s community-embedded model.
-
Frontline implementers overwhelmingly support CMHRP, with nearly universal agreement that the program improves outcomes, is acceptable to Medicaid clients and staff, and aligns with local health department missions; however, confidence in long-term sustainability is markedly lower.
-
The January 2027 Medicaid policy transition represents a critical inflection point: while standardized pregnancy risk screening will continue, changes in contracting, incentives, and service transfer processes risk weakening the linkage between screening and timely, relationship-based care management, particularly in rural and resource-limited areas.
Conclusion
North Carolina’s CMHRP Program represents a rare convergence of evidence, practice, and workforce support. Universal pregnancy risk screening, when paired with sustained, relationship-centered care management delivered through LHDs, has produced a program that is overwhelmingly viewed as effective, acceptable, and mission-critical. The evidence summarized in this brief, including findings on neonatal and maternal outcomes, suggests that the intensity and relational nature of CMHRP are central to its success.
The 2026 Medicaid policy transition does not diminish the importance of CMHRP; rather, it heightens the stakes. While standardized screening will continue, its benefits will only be realized if policy choices preserve the downstream care-management response, particularly for individuals facing social and structural barriers to care. Without deliberate action, changes in contracting and resource allocation risk eroding the very features that make CMHRP effective, especially in rural and underserved communities.
North Carolina has an opportunity to lead by demonstrating how a state can transition Medicaid care management structures while protecting a proven, community-embedded maternal health intervention. Doing so will require intentional policy design that preserves patient-centered, relationship-based care and ensures that universal risk screening continues to translate into meaningful, timely support for those who need it most.
Funding
This work did not receive any financial support.
Conflicts of Interest
The authors report no conflicts of interest.
Correspondence
Please send correspondence to Dr. Monisa Aijaz, 1601 E. Market Street, Greensboro, NC 27411 (maijaz@ncat.edu).