Introduction
North Carolina’s nursing workforce conversation often starts and ends with registered nurses (RNs).1,2 That framing is understandable—RNs anchor hospital care and many community settings—but it is incomplete for a state facing simultaneous pressures: population growth, accelerated aging, a rising burden of chronic disease, and persistent rural access gaps.1,3 In practice, the “pinch points” in care delivery are frequently in settings that rely heavily on licensed practical nurses (LPNs): skilled nursing facilities, assisted living, home health agencies, correctional health programs, behavioral health facilities, and small rural hospitals and clinics.4–6 When LPN vacancies climb, the effects are immediate—reduced admissions capacity, delayed discharges, diminished continuity, and burnout that pushes more clinicians out of the workforce.5,6
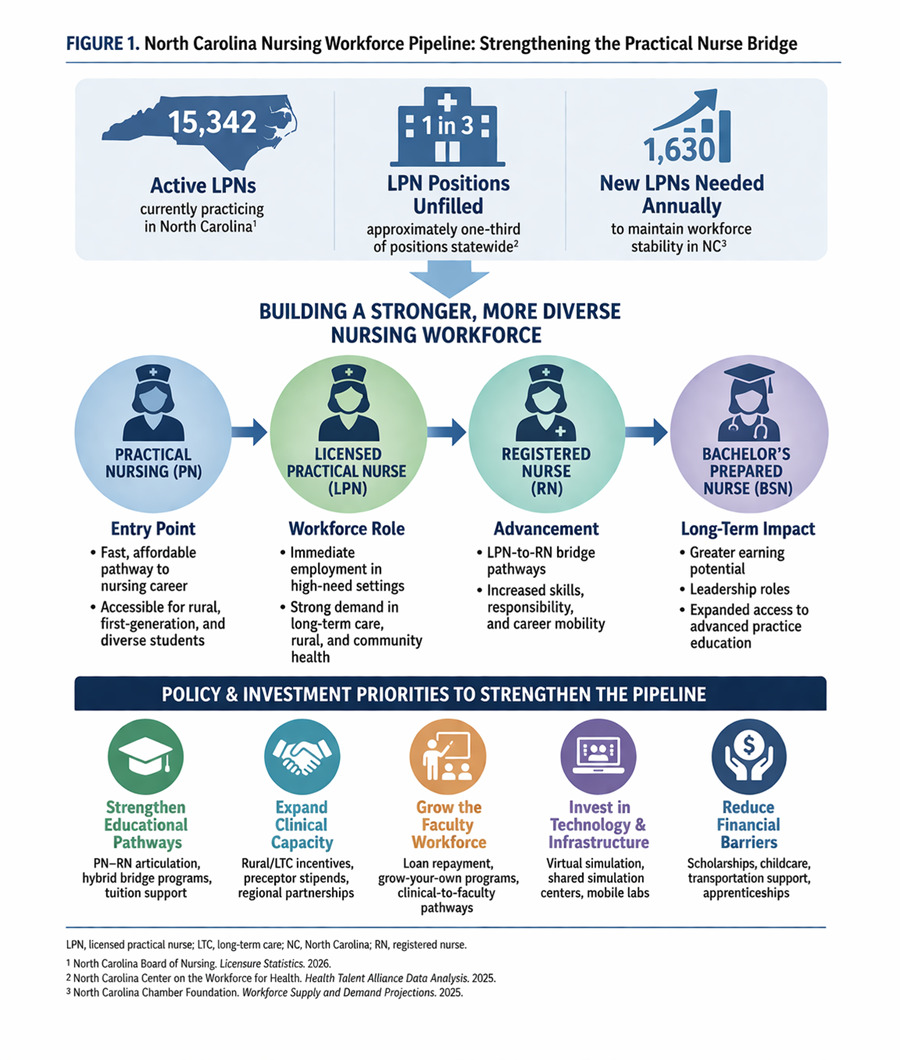
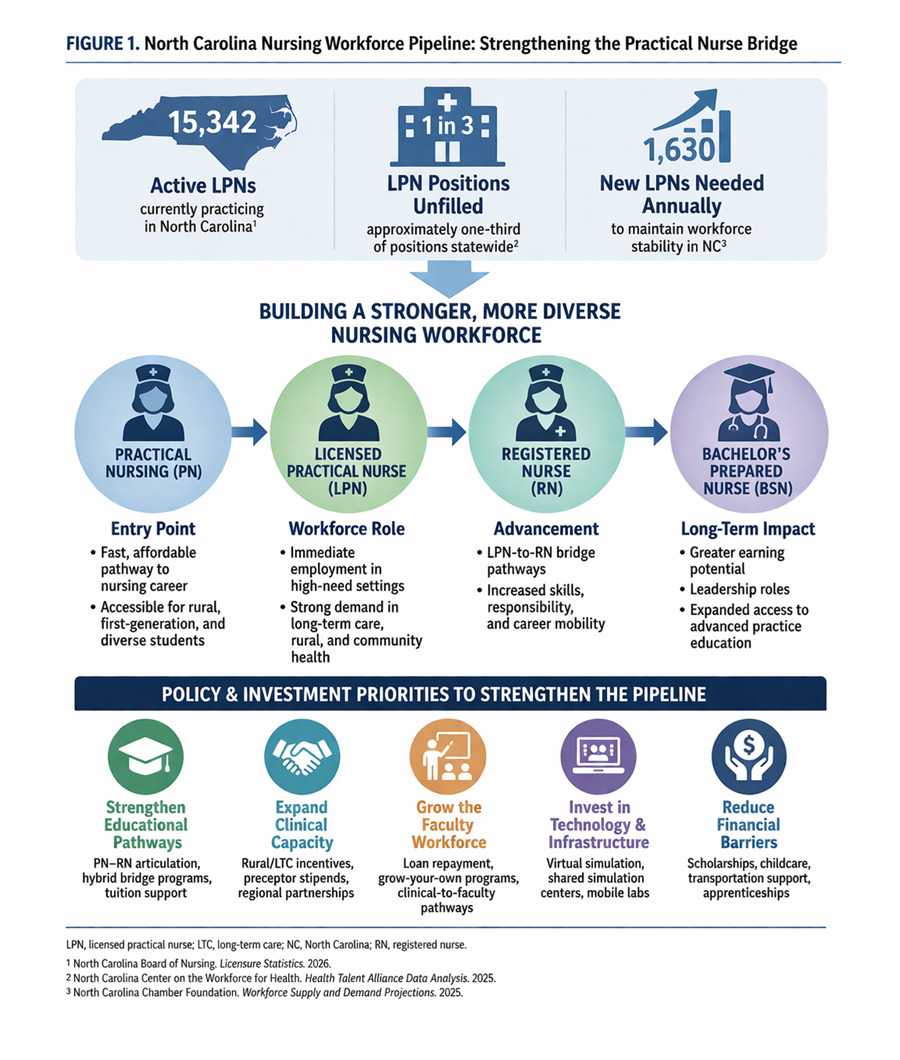
Practical nursing (PN) education—typically delivered through community colleges and regional training programs—represents an underused but highly scalable workforce lever.4,5 PN programs can place graduates into the workforce more quickly than traditional RN routes, and they can do so while widening opportunities for working adults and rural learners.4,5,7 The purpose of this commentary is to: (1) describe why LPN supply and stability are central to North Carolina’s care capacity; (2) highlight PN education as an “essential bridge” into nursing and upward mobility; and (3) recommend state and regional actions to modernize PN training, expand clinical placement capacity, and strengthen stackable pathways from LPN, to RN, to a Bachelor of Science in Nursing (BSN) (Figure 1).5,7,8
The Workforce Landscape
North Carolina’s workforce shortages are not evenly distributed.1,5 Facilities serving older adults and people with complex, chronic conditions, especially in rural counties, report persistent vacancies and high turnover among front-line nursing staff.2,5 LPNs are central to staffing models in long-term care and many community-based services, so instability in this workforce reverberates across the continuum of care.5,6 Recent North Carolina workforce assessments have reported LPN open position rates in the range of roughly one in five positions and exceptionally high “churn,” reflecting rapid movement into and out of roles and across employers.9 In some sectors, including behavioral health and long-term care, annual churn has been reported to approach or exceed the size of the workforce, implying that organizations must hire at near-constant rates simply to maintain baseline staffing.5
High vacancies and turnover are more than human resources problems; they are access and safety problems.5,6 When long-term care facilities cannot staff adequately, hospital discharge is delayed, emergency departments back up, and families struggle to find appropriate placements close to home.5,6 When home- and community-based providers cannot recruit and retain nursing staff, medically complex patients experience disruptions in medication administration, wound care, and chronic disease management.5,6 In rural regions, where alternative providers and facilities are limited, staffing volatility can translate directly into fewer beds, fewer admissions, and longer travel distances for care.1,5
PN Education as a Driver of the Workforce
A licensed practical nurse (PN) is a nurse who provides basic patient care under the supervision of a Registered Nurse.4,10 PN programs function as a labor force driver because they are designed for speed, affordability, and local alignment.4,5 Most PN programs can be completed in about a year of full-time study, and many are structured to accommodate working adults through evening, weekend, or hybrid formats.4,5 For students who cannot pause employment for a multi-year degree, PN education provides a realistic entry point into nursing with the potential for wage gains and career stability.4,5,7 For employers and communities, PN graduates can be deployed more rapidly into high-need settings including long-term care, home health, and rural clinics, where staffing shortages are often most acute.5,6
Just as important, PN education is an equity strategy.1,5,7 LPN cohorts are often more representative of the communities they will serve than the RN workforce overall, reflecting higher participation by rural students, first-generation college students, and learners balancing caregiving responsibilities.1,5,7 In a state where many rural counties struggle to “grow their own” clinicians, PN programs can anchor local pipelines: students train close to home, complete clinical experiences in nearby facilities, and are more likely to remain in the region after graduation.5,7
Emphasizing PN education is not an argument to substitute LPNs for RNs or to dilute professional standards.2,8,10 Rather, it is a recognition that the nursing workforce is a team, and that appropriate skill mix—supported by clear role delineation, adequate supervision structures, and opportunities for advancement—can stabilize care delivery.2,8,10 When LPN roles are intentionally integrated and supported, organizations can reduce avoidable turnover, strengthen continuity, and create “earn-and-learn” ladders that retain talent within nursing.5,6,8
Policy Priorities
What would it look like to treat PN education as a core component of North Carolina’s workforce strategy? The answer is not a single program or appropriation. It is a coordinated set of actions that expands training capacity while improving completion, job placement, and long-term retention.5,7,8 The priorities below and summarized in Table 1 build on what educators and employers already know: students need affordable pathways, programs need faculty and clinical placements, and employers need predictable pipelines paired with supportive work environments.5,7,8 Policy can align incentives, remove bottlenecks, and fund the infrastructure required to scale high-quality PN education statewide.5,7,8
1. Strengthen Stackable Pathways (LPN-to-RN-to-BSN)
North Carolina does not need to choose between rapid entry and long-term professional advancement; it can design for both.5,7,8 Stackable pathways allow learners to begin as LPNs, build experience and income, and then progress through bridge options to RN and BSN preparation.7,8 For communities that have difficulty recruiting nurses from outside the region, this “grow your own” model matters: learners who can remain employed locally while advancing are more likely to stay in place, strengthening regional stability.5,7
-
Create and continuously update statewide articulation agreements so that PN coursework transfers predictably into Associate Degree in Nursing (ADN) and BSN pathways.7,8
-
Expand hybrid LPN-to-RN bridge options that minimize time away from work, paired with robust advising and academic coaching.7,8
-
Incentivize employer-supported tuition, paid study time, and schedule flexibility, especially in long-term care and home- and community-based services where turnover is most destabilizing.5–7
2. Expand Clinical Capacity Through Academic–Practice Partnerships
Even when student demand is strong, PN programs cannot expand without clinical placements and qualified preceptors.5,7 North Carolina’s clinical training capacity is constrained by the same staffing shortages that PN education is meant to address; busy units and facilities may have limited time to onboard students, and preceptors may not be compensated for the additional workload.5,7 Solving this mismatch requires shared responsibility across education, employers, and the state.5,7,8
-
Regional placement collaboratives: Convene community colleges, health systems, and long-term care providers to coordinate schedules, reduce competition for sites, and optimize capacity across counties.5,7
-
Preceptor support: Provide stipends, continuing education credit, and recognition programs; consider state-supported preceptor incentives in high-need regions and sectors.5,7
-
Shared faculty models: Support joint appointments that allow experienced clinicians to teach part time while maintaining practice roles, easing faculty shortages and strengthening employer alignment.7,8
-
Purposeful diversification of sites: Normalize high-quality clinical learning in long-term care, home health, correctional health, and behavioral health—settings where LPNs are often most needed.5,6
3. Grow and Retain the Nurse Educator Workforce
Faculty capacity is a recurring limit across nursing education, including PN programs.2,7,8 Competitive clinical salaries can outpace educator compensation, and rural programs may struggle the most to recruit and retain qualified instructors.2,7 Strengthening PN education therefore requires workforce strategies for educators, not only for students.7,8
-
Grow-your-own educator tracks: Create supported pathways for experienced nurses to transition into teaching through part-time graduate coursework, mentorship, and supervised teaching experiences.7,8
-
Loan repayment and scholarships: Expand state and employer programs that reduce financial barriers for nurse educators who commit to teaching in high-need regions.7,8
-
Competitive compensation strategies: Use joint appointments, salary supplements, or differential pay for hard-to-staff geographies and specialties.7,8
-
Faculty development infrastructure: Invest in training for simulation, hybrid pedagogy, and competency-based assessment so that scaling efforts maintain quality.7,8
4. Modernize PN Education with Simulation and Flexible Delivery Without Compromising Quality
North Carolina can expand training capacity by pairing traditional clinical experiences with high-quality simulation and flexible delivery models.7,8 Simulation-enhanced learning can reduce pressure on limited clinical sites, standardize exposure to essential skills, and improve readiness for practice.7,8 Hybrid course delivery, especially for didactic content, can also widen access for rural learners who would otherwise face long commutes or relocation.5,7
Investments in shared regional simulation centers and mobile simulation resources can extend training infrastructure beyond major metropolitan campuses, particularly when paired with faculty development and common evaluation tools.7,8 At the same time, expansion must be disciplined: simulation should complement—not replace—meaningful clinical experiences; programs should track licensure pass rates, completion, and early-career retention; and employers should provide feedback loops on graduate readiness.7,8,10 The goal is scale with integrity: more seats, more graduates, and strong preparation for the settings where LPNs will practice.5,7,8
5. Reduce Financial Barriers and Support Completion
Because PN education attracts many working adults, completion depends as much on logistics as on academics.5,7 Tuition and fees matter, but so do transportation, child care, technology access, and the ability to reduce work hours during intensive clinical rotations.5,7 If North Carolina wants PN programs to function as a reliable workforce engine, the state should treat wraparound supports as core infrastructure rather than optional add-ons.5,7,8
-
Targeted scholarships and last-dollar grants for PN students committing to work in high-need settings or regions after licensure.5,7
-
Paid apprenticeship or learn-and-earn models that allow students to remain employed while progressing through training, with clear role boundaries and supervision.5,7,8
-
Student support services, including child care partnerships, transportation assistance, emergency aid, and proactive advising.5,7
-
Employer–education compacts that link tuition support to retention strategies such as residency-style onboarding, mentorship, and predictable scheduling.5,7,8
Measuring Success: Metrics That Matter to Communities
Workforce investments should be evaluated with measures that reflect both educational performance and health system impact.5,7,8 Beyond enrollment counts, the state should monitor whether PN education expansions translate into stable staffing in the settings that most influence access—long-term care, home- and community-based services, behavioral health, and rural facilities.5,10
-
PN program applications, enrollment, completion, and National Council Licensure Examination for Practical Nurses (NCLEX-PN) pass rates.
-
Time-to-hire and vacancy rates for LPN roles by sector and region.
-
One-year and two-year retention of newly licensed LPNs in North Carolina.
-
Progression rates from LPN-to-RN and RN-to-BSN pathways.
-
Placement patterns in rural counties and high-need settings.
-
Downstream indicators such as delayed hospital discharges are attributable to long-term care capacity constraints.
Conclusion
PN education is one of the most immediate, scalable strategies available to strengthen North Carolina’s health care workforce—particularly in places where access is most at risk.5,7 By treating PN programs as a strategic workforce asset, the state can expand entry into nursing, stabilize long-term care and community-based services, and build upward mobility pathways that retain talent.5,7,8 The next step is coordinated investment: align education and employer incentives, expand clinical and faculty capacity, modernize delivery with quality safeguards, and reduce the financial friction that prevents students from completing.5,7,8 Strengthening this “essential bridge” is not just a pipeline solution; it is a commitment to keeping care close to home for North Carolinians.5
Declaration of Interests
The author has no conflicts of interest to declare.
Correspondence
Address correspondence to Lori Hayes Byrd, UNC Chapel Hill School of Nursing, Campus Box 7460, Chapel Hill NC 27599 (loribyrd@unc.edu).