Introduction
Healthy aging is commonly associated with maintaining a healthy weight through exercise and balanced nutrition, staying on top of preventive care by scheduling annual physical exams and vaccinations, and avoiding harmful substances. In addition to these factors, psychosocial aspects of healthy aging, such as adequate social engagement and good mental health, are increasingly viewed as having a tremendous impact on one’s well-being.
Social isolation has a significant negative impact on an individual’s mortality from all causes comparable to the negative impacts of smoking, obesity, and lack of exercise; the negative impact of social isolation is akin to smoking 15 cigarettes per day.1 Loneliness, or the subjective feeling of being isolated, has been associated with many negative health impacts, including higher rates of clinical depression, anxiety, and suicidal ideation.2 Perissinotto and colleagues in 2012 found loneliness to be associated with a 59% increased risk of functional decline and a 45% increased risk of death.3 Poor social relationships have been associated with increased risk of coronary heart disease and stroke.4 Finally, social isolation has been associated with an increased risk of developing dementia.5 Efforts to highlight the importance of addressing social isolation and loneliness as public health problems worthy of serious attention are underway in North Carolina,6 across the United States, and in countries across the world.
In 2017, AARP produced a report on the financial impact of social isolation among older adults. This study examined Medicare spending data and found that the additional monthly cost to Medicare for a socially isolated enrollee was $134, higher than the cost of arthritis ($117) and approaching the cost associated with high blood pressure ($163).7 Overall, a lack of social contacts was associated with a $6.7 billion increase in federal health care spending.7 US Surgeon General Vivek Murthy has repeatedly spoken out about the social isolation and loneliness epidemic.8 Other nations, such as England and Japan, have prioritized addressing social isolation and loneliness by establishing top-level government positions charged with tackling the complex issue.9–11
Older adults are more likely to be socially isolated.12 As a person grows older, their number of connections typically declines, though there is some evidence that frequency of socializing, religious participation, and volunteerism increase with age.13 The COVID-19 pandemic spotlighted the issue of social isolation and loneliness, especially among the aging population, who were at greatest risk of hospitalization and death from the virus.14,15
DAAS Response to the COVID-19 Pandemic
Promoting Social Connection
North Carolina is rich with resources to help older adults remain connected and engaged. For decades, the North Carolina Division of Aging and Adult Services (DAAS) has been at the forefront of addressing social isolation and loneliness through its extensive network of home- and community-based services. Together with North Carolina’s 16 area agencies on aging and over 500 local provider agencies, DAAS offers over 170 senior centers where older adults can participate in a variety of programs, and at least twice as many congregate nutrition sites where they can receive a hot meal in communion with others. North Carolina’s aging-service providers also provide support programs, health promotion programs, numerous volunteer opportunities, and many other programs that help connect older adults to other people.
Of particular importance is North Carolina’s senior center model, which operates through a unique combination of staff training and senior center certification. In 2017, DAAS examined the outcomes of senior center participation through a survey of over 7000 North Carolina senior center participants. Survey respondents overwhelmingly reported a positive impact on well-being, learning, management of health, support systems, creativity, access to services, and self-advocacy skills.16 Specific to social isolation, respondents reported increased volunteerism and decreased loneliness and feelings of isolation.16 Between July 2021 and June 2022, DAAS estimates that North Carolina senior centers served over 148,000 older North Carolinians.
When the COVID-19 pandemic began, senior centers were forced to shut down. Many senior center staff began offering virtual classes as an alternate means of helping older adults remain connected. In early 2021, DAAS instituted a new requirement that certified senior centers offer live phone-based or internet-based opportunities for participants to interact with other people. This requirement should remain in place regardless of the pandemic, because it helps reach those in the community who cannot physically attend senior centers for a variety of reasons.
DAAS partnered with the North Carolina Center for Health and Wellness (NCCHW) to build upon a statewide health promotion initiative (Healthy Aging NC or HANC) and create a statewide platform for virtual senior center and other social engagement programs. This effort expanded to include a variety of social engagement resources, an online social connectedness and loneliness self-assessment tool, and the opportunity to be connected to one-on-one assistance.
Addressing Mental Health Challenges
Every 58 minutes, an older adult dies by suicide in the United States, and 5–25 times more incidences of suicide exist in this population than what is reported.17,18 Though older adults represent 16% of the US population, they represent 18.8% of all deaths by suicide; in 2018, the suicide rate for those over age 65 was 17.4 per 100,000, compared to national rate of 14.8 per 100,000.17 In North Carolina, the suicide rate among older adults was 16.2 suicides per 100,000 population compared to 15.6 per 100,000 for all ages.19
In 2020, DAAS connected with two university researchers who focus on the relationship between social isolation, loneliness, and elevated suicide risk: Dr. Matthew Fullen of Virginia Tech and Dr. Laura Shannonhouse of Georgia State University. Together they conducted a statewide survey examining service providers’ experience with, and capacity to address loneliness due to social isolation, mental health issues, and elevated suicide risk. This unpublished survey showed that service providers felt the gravity of the issues faced by the seniors in their communities far outpaced their capacity to address them.
In July/August of 2022, DAAS partnered again with Fullen and Shannonhouse to address the capacity issue that was identified in the previous survey. Together they offered a two-part training based on the BE WITH (Belonging & Empathy With Intentional Targeted Helping) approach to 67 individuals statewide. The first part included a new virtual program developed with funding from the Administration on Community Living based on research showing that all people want and need to belong, that thwarted belongingness is a key risk factor for suicide, and that even one important connection can create a sense of belonging. The goal of BE is to help build empathy skills, which in turn allows staff to help people feel they belong. Part two was the Applied Suicide Intervention Skills Training (ASIST), a two-day, 14-hour standardized suicide first-aid training that is included in the Substance Abuse and Mental Health Services Administration (SAMHSA) evidence-based intervention registry and used in crisis centers across country.
The researchers examined the effectiveness of providing the ASIST training to aging-service professionals and found improvements in three key areas: comfort, competence, and confidence to intervene with a person at risk of suicide. Participants also demonstrated statistically significant improvements in level of skill. Feedback was overwhelmingly positive. Participants shared the following quotes:
“It was one of the best trainings I have ever been to. I am leaving feeling like I can actually do something for people with mental illness and suicidal thoughts. There is hope now.”
“This program is wonderful and gave participants the tools to meet the needs of our clients.”
“It has been a wonderful training opportunity and if we can even be preventing one suicide completion then we have been successful.”
Healthy Aging Task Force
Another major initiative of 2022 was the launch of the North Carolina Institute of Medicine Task Force on Healthy Aging, which convened stakeholders from across the state to look at four major issues related to healthy aging based on the Association of State and Territorial Health Officers recommendations20: falls and injury prevention, nutrition and food security, mobility, and social isolation. Later this year, the task force will make recommendations to key state decision-makers for improving these four areas.
New and Ongoing Initiatives
DAAS plans to focus on two key initiatives in 2023: 1) Continue promoting social connection by expanding the partnership with the NCCHW and the HANC social engagement web resources and addressing digital equity; 2) Expand and sustain a caregiver initiative.
Social Connection
DAAS plans to extend its work with the NCCHW to continue refining the resources on the HANC platform, and to support another social isolation program initiated by the NCCHW. This “Social Bridging Project” pairs student volunteers with older adults who are socially isolated. Volunteers are trained to help people access resources—including those that address digital equity—and provide social support by talking and listening. A 2021 evaluation of the Social Bridging Project shows promise as most participants reported decreased loneliness and increased connectedness.21 The HANC platform needs to be further developed, promoted, and eventually equipped to allow for referrals to local staff and resources for those who are socially isolated.
Digital Equity
Addressing digital equity—defined by the US Office of Educational Technology as the condition in which all individuals and communities have the internet technology capacity needed to participate fully in society—is critical.22 The pathway to digital equity is “digital inclusion”—activities needed to ensure all have access to and use of information and communication technologies, including affordable broadband, internet-enabled devices, and access to digital literacy training, technical support, and materials to encourage self-sufficiency over time.22
DAAS plans to contract with professionals to develop a digital navigator curriculum and use recently awarded grant funding to hire and train digital navigator master trainers. These trainers will be strategically located throughout the state to train lay leaders in best practices for providing digital navigation skills to older North Carolinians and build out other resources to promote digital inclusion.
Caregiver Support
In North Carolina, more than 1 in 6 adults identify as caregivers, and 356,000 caregivers are providing care to those living with Alzheimer’s, which equates to over $7.26 billion in unpaid care annually.23 The role of caregiving creates additional challenges to social engagement. During the pandemic, DAAS piloted a program called Trualta, a virtual caregiving resource that caregivers can access from the comfort of their homes at a time that works best for them. Since the program launched in North Carolina, over 1030 caregivers have joined. This program shows a lot of promise for addressing the many complex needs of caregivers.
Recommendations
National Recommendations for Addressing Loneliness and Social Isolation
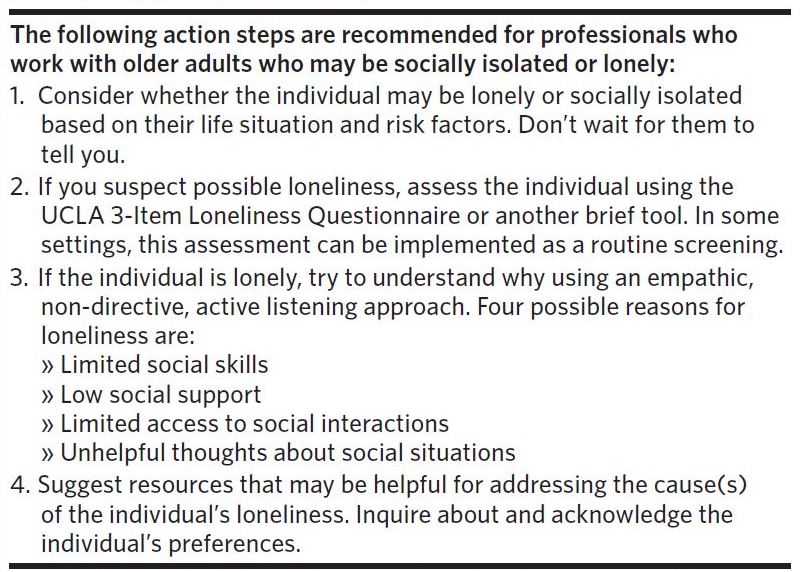
Research demonstrates inconsistent evidence of effectiveness of most interventions aimed at addressing social isolation and loneliness. In July 2020, the Suicide Prevention Resource Center (SPRC) published “Reducing Loneliness and Social Isolation among Older Adults,” which identified three key steps for reducing loneliness and social isolation.16 The report notes that it is important to recognize that loneliness has different causes and match the approach to the unique needs and preferences of the individual. Table 1 provides a summary of SPRC’s proposed action steps, reflecting this individualized approach.

Recommendations to the Department of Health and Human Services
In 2021 DAAS had the opportunity to host two graduate students, Will Shipman and Keren Hendel, who examined the issue of social isolation and loneliness more closely. Over the course of two semesters, the students completed an environmental scan—including a thorough analysis of the survey completed the year prior—examined existing screening tools, conducted interviews with key departmental leaders, and presented to and hosted a guided discussion with key departmental leaders.
Three recommendations were made in an unpublished report to the North Carolina Department of Health and Human Services (NCDHHS): 1) Create a task force to address social isolation, loneliness, and elevated suicide risk; 2) Incorporate the UCLA 3-item loneliness scale into Medicaid home- and community-based services screen tools and the NCCARE360 platform, and build referral pathways to existing social engagement resources, which should expand over time; 3) Fund community efforts and pilots through grants, particularly those that support high-need groups.
Other Recommendations
Staff from the North Carolina Center for Health and Wellness contributed a chapter in Geriatric Medicine and Healthy Aging titled “Social Distancing and Isolation: Unintended Consequences, Concerns, and Antidotes for Older Adults.” In this chapter, they make several key recommendations: 1) Social isolation and its antidote, social connectedness, should be recognized as a social determinant of health and should be a consideration in health policy decisions; 2) Human service organizations, policymakers, governmental, and private foundation funders should prioritize programmatic opportunities to increase social connection for older adults; 3) Medical providers and health teams should build on efforts to reach people in their homes or communities with whole-person medical and health care; and 4) Broad public (community and governmental) support for infrastructure and technology access and education projects is needed.6
Conclusion
Social isolation and loneliness are important public health issues that require attention. While older adults are the focus of many recent initiatives, these issues can impact anyone. There are many efforts underway that should be supported and expanded upon. Much work is still needed in the public sector including implementing policy and programmatic solutions.
Author Bio
Rebecca Freeman, MPH human service planner/evaluator, North Carolina Division of Aging and Adult Services, Raleigh, North Carolina.
Disclosure of interests
The author reports no disclosures.