
Coronavirus disease 2019 (COVID-19), caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is associated with a high incidence of thrombotic complications.1–3 The pathogenesis of SARS-CoV-2 leading to thrombosis involves an aggressive inflammatory response known as the cytokine storm, endothelial cell injury, and activation of platelets and clotting factors, resulting in a hypercoagulable state.3 An autopsy study of patients who died of acute respiratory distress syndrome (ARDS) in the setting of COVID-19 early in the pandemic revealed that COVID-19 patients had a 9-fold greater prevalence of alveolar capillary microthrombi compared to patients who died of ARDS in the setting of influenza.4 An indicator of this inflammatory and hypercoagulable state is thought to be elevated levels of D-dimer, a degradation product of cross-linked fibrin.1,5,6
In response to the potential for thrombosis in patients with COVID-19, both prophylactic (low) and therapeutic (high) doses of antithrombotic drugs have been administered. Antithrombotic drugs are divided into 3 classes— anticoagulants, antiplatelets, and fibrinolytics—each having a distinct mechanism of action. Fibrinolytics act to dissolve existing clots, whereas anticoagulants and antiplatelets prevent thrombosis by inhibiting clotting factors of the coagulation cascade or platelet aggregation, respectively.7,8 Recent guidelines recommend prophylactic doses of anticoagulants such as heparin for the management of COVID-19 based on trials with both prophylactic and therapeutic anticoagulation treatment arms.9,10 For example, a recent trial of therapeutic anticoagulation with heparin in non-critically ill patients with COVID-19 showed that therapeutic anticoagulation with heparin is associated with a greater probability of survival, hospital discharge, and a greater number of days free of cardiovascular or respiratory organ support compared to prophylactic anticoagulation with heparin.11 In contrast, trials using similar treatments (therapeutic anticoagulation with heparin) in critically ill patients with COVID-19 did not demonstrate a survival benefit.12,13 The role of fibrinolytics and antiplatelet agents as treatments for COVID-19 is not yet clear, but several clinical trials with antiplatelet drugs, such as aspirin and clopidogrel are ongoing (NCT04409834, NCT04424901, and NCT04505774).14
Minority and rural populations experience greater risk for severe COVID-19 illness and mortality and appear underrepresented in COVID-19 research.15 In the context of these findings, we sought to analyze the incidence of thrombotic complications among the largely rural population of Cumberland County, North Carolina, and surrounding area, which is home to few major urban centers.16 Fayetteville is the largest city within this region and is home to Cape Fear Valley Medical Center, a 678-bed tertiary care hospital. Therefore, the goal of this study was to analyze patient records from the Cape Fear Valley Medical Center to: 1) determine the prevalence and impact of thrombosis in patients with COVID-19 in rural areas of North Carolina and 2) identify potential interventions associated with improved outcomes in this patient population.
Methods
This retrospective case-control study utilized deidentified records collected from 2237 patients at the Cape Fear Valley Medical Center in Fayetteville, North Carolina, from March 2020 to January 2021. This research was approved as an exempt protocol by the IRB of the Cape Fear Valley Medical Center (protocol #326-20) prior to data collection. Data included demographic characteristics, discharge disposition, thrombosis, antithrombotic drug treatment, ICU admission, ventilation, and terminal diagnosis, which was defined as either death or hospice care utilization. We created binary (yes/no) variables for the primary endpoints of terminal diagnosis, death, ICU admission, ventilation, and receipt of any medication (heparin, enoxaparin, warfarin, apixaban, rivaroxaban, clopidogrel, ticagrelor, and prasugrel), anticoagulant medication (heparin, enoxaparin, warfarin, apixaban, and rivaroxaban), and antiplatelet medication (clopidogrel, ticagrelor, and prasugrel). Based on literature values, we defined a high/low D-dimer variable (2 μg/mL).
A number of patients had multiple records in the dataset (corresponding to multiple hospital visits within the study period). Out of the 2727 records in the original data from 2237 patients, 490 visits were distributed across 375 patients with a range of 2–7 records per patient. In an attempt to eliminate bias and make those with multiple records comparable to those with just a single record, we created a set of rules (without inspecting the data). For each patient with multiple records: 1) any incidence of death, hospice care, ICU admission, or thrombosis was counted and retained; 2) medications from only the most recent admission date were counted in the single row, which was retained (medications from all other rows were excluded); and 3) D-dimer values from a patient’s initial (oldest) visit were retained (D-dimer values from all other rows were excluded).
Multivariable logistic regression models were constructed to evaluate the relationship between thrombosis and each outcome of terminal diagnosis, ICU admission, and ventilation. Age was included as a predictor variable in each model to account for concerns over any confounding between thrombosis and age. Odds ratios (OR) and associated 95% confidence intervals (CIs), adjusted for the inclusion of age in each model, were reported.
Computation of unadjusted ORs and 95% CIs permitted an assessment of the strength of the relationship between 1) terminal diagnosis and various medication use as well as ICU admission and various medication use (any medication, anticoagulant medication, and antiplatelet medication); 2) death or ICU admission and D-dimer level (low versus high) overall as well as amongst those with only thrombosis; and 3) death or ICU admission and (combined) thrombosis and high D-dimer level (both versus not both).
We conducted 2 sample independent group t-tests to compare the mean D-dimer values for those with and without thrombosis. Subjects missing data were excluded only from analyses for which the data were missing. As this was an exploratory, hypothesis-generating type of study, no adjustments for multiple comparisons were made. In addition, following current thinking regarding best practices for significance testing, P-values were reported as appropriate, but statistical significance was not evaluated for any results.17 All analyses were generated using SAS version 9.4 or JMP version 14.
Results
The purpose of this retrospective single-site study was to identify potential associations between COVID-19 and thrombosis with respect to patient outcome, antithrombotic strategies, and disease severity in a hospitalized population from a rural demographic. To evaluate the association of thrombosis with these factors, 2237 patients were divided into 2 groups for further analysis: case (COVID + thrombosis, n = 97) and control (COVID-19 alone, n = 2140). All 2237 patients were SARS-CoV-2 positive, predominantly female (52.9%), and mostly identified as either African American (52.1%) or White (32.7%, Table 1). The Cape Fear Valley ICU admitted a relatively low number of patients (8.6%) from our cohort and a similar number received ventilation treatment (7.8%). Only 97 COVID-19-positive patients were diagnosed with cardiovascular or cerebrovascular thrombosis (4.3%) as defined by clinical evaluation and diagnosis-related group (DRG) codes. However, 20.6% of those needing intensive care were diagnosed with thrombosis (Table 1. Overall, patients experienced a variety of outcomes, with the vast majority surviving and discharged to home (1611, 72.0%), whereas 247 patients (11.1%) expired or received hospice care. Patients who left against medical advice or were discharged to long-term care collectively represented 2.0% of the total population studied (Table 1).
Impact of Thrombosis
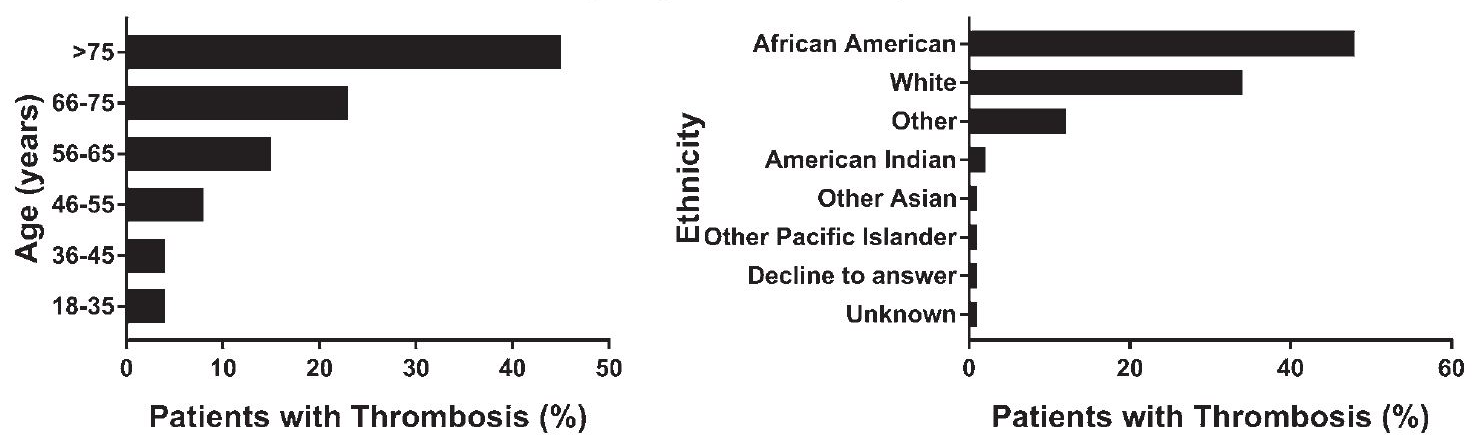
To evaluate the impact of thrombosis on patient outcomes and epidemiology, odds of terminal diagnosis (death or hospice), ICU admission, and initial D-dimer levels in thrombotic (case) and nonthrombotic COVID-19 patients (control) were analyzed. Over 80% of thrombotic patients were aged 56 years or over, with the highest fraction of thrombosis occurring in patients over age 75, at 45.4% (Figure 1A). Reflective of the total COVID-19-positive patient population in this study, 47.9% of thrombotic patients were African American, followed by 34.4% who were White, with the remaining 17.7% of other ethnicities (Figure 1B).
_or_(b)_ethnicity.png)
Thrombosis in combination with COVID-19 was associated with a higher risk of terminal diagnosis compared to patients with COVID-19 alone after adjusting for age (OR 1.81, 95% CI 1.10–2.97, Table 2). In addition, patients with thrombosis were more likely to be admitted to the ICU (OR 2.25, 95% CI 1.33–3.81, Table 2) or placed on a ventilator (OR 2.46, 95% CI 1.45–4.18, Table 2). These data indicate that a combination of thrombosis and SARS-CoV-2 infection greatly influences patient outcome with respect to increased probability of mortality and severity of disease, even after accounting for age in each model.
D-dimer
Despite this strong correlation between thrombosis and adverse outcomes, levels of the clot biomarker D-dimer only weakly correlated with thrombosis. As shown in Figure 2, among 1176 patients who underwent laboratory-confirmed D-dimer testing, the mean D-dimer value for 62 thrombotic patients was 4.0 ± 6.52 μg/mL compared to 2.24 ± 3.82 μg/ mL for 1114 patients without thrombosis (Figure 2, P = .04).

To further analyze D-dimer levels, a “high” D-dimer value was derived from the literature (≥ 2 μg/mL) and used as a threshold value to assess the association between D-dimer level (high, ≥ 2 μg/mL versus low, < 2 μg/mL) and death. High D-dimer was associated with an increased risk of death irrespective of thrombosis (OR 2.92, 95% CI 2.09–4.10, Table 2).
Thrombosis incidence was calculated as a percentage of patients within the indicated age ranges (A) or ethnicity (B). Only data for thrombotic patients are shown for both panels (n = 97). Thrombosis across ethnicity closely mimicked the racial distribution of the entire patient population (N = 2237).
However, the risk of death within the thrombotic case population alone was not found to be associated with D-dimer level (OR 0.88, 95% CI 0.28–2.78, n = 62, Table 2) nor did the combination of thrombosis and high D-dimer level associate with increased risk of death within the total population (data not shown). Collectively, our data show a weak correlation between thrombosis and high D-dimer level despite the similar maximum D-dimer values for thrombotic and nonthrombotic COVID-19 patients. High D-dimer value correlates more strongly with death in the total population, which is driven by the higher number of nonthrombotic COVID-19 patients in this cohort.
Antithrombotic Treatment
In an effort to determine which anticoagulant treatment strategies were associated with positive outcomes, odds of terminal diagnosis and ICU admission were calculated in patients given anticoagulant medications. Antithrombotics were broadly defined as either anticoagulant (heparin, enoxaparin, warfarin, apixaban, and rivaroxaban) or antiplatelet (P2Y12 antagonists: cIopidogrel, ticagrelor, and prasugrel) medications. Over 61% of all patients and 91.8% of thrombotic patients received at least 1 anticoagulant or antiplatelet medication. The majority of thrombotic patients received anticoagulants (55.7%) as opposed to antiplatelet drugs alone (1.0%) or a combination of both (35.1%).
Admission to the ICU indicated disease severity. Patients receiving at least 1 antithrombotic drug were more likely to be admitted to the ICU (OR 10.54, 95% CI 5.84–19.04, Table 3). Patients receiving an antiplatelet drug (as compared to those who received none) were also more likely to arrive in the ICU (OR 1.88, 95% CI 1.17–3.03, N = 2237, Table 3) but with relatively lower odds.
Similarly, odds of terminal diagnosis (defined as in-hospital death or discharged to hospice care) for patients receiving at least 1 type of antithrombotic medication as compared to those receiving none, regardless of thrombotic status, was very high (OR 12.13, 95% CI 7.02–20.96, Table 3). Patients receiving at least 1 anticoagulant (as compared to those receiving none) experienced high odds of terminal diagnosis (OR 12.33, 95% CI 7.14–21.30, Table 3). Interestingly, the odds of terminal diagnosis in patients receiving at least 1 antiplatelet medication compared to patients receiving no antiplatelet medications (anticoagulants alone) was relatively low (OR 2.30, 95% CI 1.52–3.48, Table 3). Furthermore, of the 23 thrombotic patients who died, 60.9% were treated only with anticoagulants, whereas 39.1% were treated with both anticoagulant and antiplatelet drugs, and none were treated with antiplatelet drugs alone. These outcomes likely reflect severity of disease, as we have no reason to believe medication(s) directly contributed to morbidity or mortality.
Discussion
Patients with COVID-19 hospitalized at Cape Fear Valley Medical Center had a 4.3% incidence of thrombosis. Compared to other studies focused on thrombosis in COVID-19 patients, this incidence appears low. Among COVID-19 patients hospitalized at the nearby Duke University Health System, 12.0% experienced a thromboembolic event,18 and among 3334 hospitalized COVID-19 patients in New York, the thrombosis incidence was 16.0%.1 Thrombotic events in COVID-19 patients in the ICU setting, however, were comparable between our cohort (20.6%) and populations from large urban areas or multicenter studies, which ranged from 6.3% to 31%.5,13,19–21
Over 80% of thrombotic patients in our study were aged 56 years or over, with the highest fraction of thrombosis occurring in patients aged over 75, which is consistent with existing data.22 This increased risk for severe disease in older patients could be due to increased susceptibility to the virus, the presence of comorbidities, and naturally waning immunity.23,24 Comparing census data for Cumberland County to our study cohort, a disproportionately large percentage of the patients were African American.25 Other studies have observed a disproportionate incidence of COVID-19 among racial minority groups, which may reflect differences in housing, work environments, or underlying medical comorbidities.15,26
While patients in this study had a relatively low incidence of thrombosis, patients with thrombosis were more likely to have severe disease (ICU admission) or require ventilation treatment. Additionally, those with documented thrombotic events were at higher risk of terminal diagnosis (death or hospice) compared to patients with COVID-19 alone. These data indicate that COVID-19-associated thrombosis greatly influences patient outcome with respect to increased probability of mortality and severity of disease and are consistent with other studies.21,27
Although considered a feature of COVID-19-associated coagulopathy, an elevated D-dimer level in our patient population only weakly correlated with thrombosis. In fact, both case and control populations in our study exhibited “high” (≥ 2 μg/mL) mean D-dimer concentrations and were not statistically different. It is well known that elevated D-dimer concentrations are observed in many thrombotic disease states, such as pulmonary embolism and deep vein thrombosis, but do not always indicate thrombosis since D-dimer values may be elevated in nonthrombotic conditions, such as pregnancy, trauma, infection, liver disease, and malignancy.28,29 However, an extremely elevated D-dimer is uniquely associated with severe disease including venous thromboembolism, sepsis, cancer, and now COVID-19.1,5,30,31 Elevated D-dimer levels also correlated with severe disease in our patient cohort, manifested by increased odds of death, which suggests that abnormally elevated D-dimer levels serve more as a general predictor of a negative patient outcome than as a specific marker for thrombosis.30,32,33
Despite patient demographics, disease severity, or a clear diagnosis of thrombosis, initiation of antithrombotic medications is becoming the standard of care for hospitalized COVID-19 patients. Heparin is the prototypical prophylactic anticoagulant used for most hospitalized patients and has been globally recommended as a treatment for COVID-19; however, some studies show therapeutic doses of heparin are insufficient for reversing the hypercoagulable state induced by COVID-19.12,13
In addition to coagulation, platelet hyperreactivity contributes to the thrombotic sequelae of COVID-19. For example, multiple groups have shown that platelets isolated from COVID-19 patients have a procoagulant or hyperreactive phenotype in which platelets secrete higher levels of activation markers such as P-selectin, aggregate more intensely in response to agonists, and generate more leukocyte-containing aggregates compared to controls.34–38 Other studies have revealed that platelet development, secretion, and regulation of normal blood clotting (hemostasis) are critical pathways affected by COVID-19.39–41 Consistent with these data, the use of antiplatelet drugs in COVID-19 patients appears to improve patient outcomes and respiratory symptoms. For example, aspirin treatment correlates with reduced all-cause mortality and severity of COVID-19 symptoms42 and fondaparinux treatment in combination with aspirin, clopidogrel, and tirofiban leads to increased arterial oxygen partial pressure and reduced hypoxemia.43
Despite these encouraging results, data regarding efficacy of antiplatelet strategies in COVID-19 remain scarce. Interestingly, patients in our study who received at least 1 antiplatelet medication compared to those receiving no antiplatelet medications (anticoagulants alone or no medications) experienced a lower risk of death and discharge to hospice care. These data indicate that anticoagulants used in this patient population only partially mitigated the odds of death or severe disease and suggest that antiplatelet drugs or a combination of anticoagulant and antiplatelet medications may be more effective treatment options compared to anticoagulants alone. Furthermore, of the thrombotic patients who died, 60.9% were treated only with anticoagulants, whereas 39.1% were treated with both anticoagulants and antiplatelet drugs, suggesting that targeting platelet activation may be beneficial for certain COVID-19 patients. In fact, another group recently identified prior antiplatelet therapy as a beneficial factor for COVID-19 outcome.44 As of this writing, there are several ongoing clinical trials investigating efficacy of anticoagulant, antiplatelet, and combinations of both in patients with COVID-19 (e.g., NCT04324463, NCT04359277, NCT04409834, NCT04424901, and NCT04505774).
A limitation of this study is the lack of medication and health history prior to hospitalization, as antithrombotic treatments and comorbidities could potentially impact outcomes and interpretation of the data. Due to the retrospective design of this study, however, it is not possible to demonstrate causal relationships between disease states and mortality, nor between therapeutic interventions and improved patient outcomes; retrospective analysis can only identify association, not causation. However, our results are consistent with another recently published retrospective antiplatelet analysis, which suggests that retrospective study designs may be valuable for identifying associations in COVID-19 patient populations.44
In conclusion, our study addresses an unmet need by evaluating the impact of thrombosis in patients with COVID-19 from rural communities and by identifying potential interventions that may benefit this patient population. The overall incidence of thrombotic complications in this cohort is relatively low, but as with other populations in more urban settings, thrombosis was associated with increased mortality and COVID-19 disease severity. Importantly, the combination of anticoagulant and antiplatelet drugs greatly lowered the odds of death and severe disease, suggesting that the addition of antiplatelet drugs to an antithrombotic treatment regimen for hospitalized COVID-19 patients may be an effective therapeutic option. Higher-powered prospective trials will be necessary to confirm our observations and the potential merits of antiplatelet therapy in these patients.
Author Bios
Swarna Reddy, MS planner and evaluator, North Carolina Division of Aging and Adult Services, Raleigh, North Carolina.
Divya Venkataganesan, MPH planner and evaluator, North Carolina Division of Aging and Adult Services, Raleigh, North Carolina.
Acknowledgments
All authors contributed to the writing of the manuscript. AB, BB, DCM, JC, and SPH created the experimental design. MRJ performed statistical analysis. AB, SPH, and DCM wrote the IRB. DCM acquired medical records. MRJ and SPH made figures.
This work was supported by the Honors College of Campbell University (AB), College of Pharmacy and Health Sciences, Department of Pharmaceutical Sciences and Clinical Research at Campbell University (MRJ, SPH), and the School of Osteopathic Medicine at Campbell University (KJ, BB, DCM, JC).
The authors declare no conflicts of interest.