Background
The COVID-19 pandemic has resulted in many adverse impacts to North Carolinians, including impacts other than those directly attributed to the SARS-CoV-2 virus and its variants. The pandemic resulted in widespread economic and social disruption, highlighting and intensifying inequalities across the life course. While protective for infectious diseases, mitigations like the stay-at-home orders exacerbated social isolation, a known risk factor for violence.1 Other shared risk factors for violence were amplified during the pandemic, such as unemployment, lack of community support or cohesion, and increases in media depictions of violence as the country was deeply affected by numerous nationally publicized violent events.1,2
Over half (56.7%) of violent deaths in the United States and over two-thirds (68.1%) in North Carolina involve a firearm.3,4 During the pandemic, the US firearm homicide rate increased, and firearm suicide rates remained high; rates in 2021 were the highest recorded for both firearm homicide and suicide since the early 1990s.5–7 Similar trends were observed in the number of firearm injury emergency department (ED) visits that occurred nationally during the pandemic, with increases coinciding with the declaration of COVID-19 as a national emergency.5
A sharp nationwide increase in firearm purchasing also occurred during the COVID-19 pandemic. An estimated 7.5 million US adult citizens became new gun owners between January 1, 2019, and April 26, 2021.8 Similar shifts in firearm purchasing occurred in North Carolina. The Federal Bureau of Investigation National Instant Criminal Background Check System reports that the number of firearm permits submitted for background check increased 67.9% from 2019 to 2020 in North Carolina.9 Data on firearm-related deaths and ED visits in North Carolina were analyzed to better understand the impacts to firearm injury morbidity and mortality in North Carolina during the COVID-19 pandemic.
Methods
The North Carolina Violent Death Reporting System (NC-VDRS) was used to analyze firearm-related deaths during 2017–2021; 2021 NC-VDRS data are provisional and subject to change (data as of March 6, 2023). Firearm-related injury ED visits were obtained from the North Carolina Disease Event Tracking and Epidemiologic Collection Tool (NC DETECT) over the same period using the NC-FASTER (Firearm Injury Surveillance Through Emergency Rooms) CDC Firearm Injury All Intents Version 2 syndromic surveillance definition.10 Data were limited to North Carolina residents. Rates were calculated per 100,000 residents overall and by demographic group using National Center for Health Statistics (NCHS) bridged population estimates; 2021 rates were calculated using 2020 population estimates as a proxy due to changes in the availability of NCHS bridged estimates. Percent change was calculated to compare firearm injury and death rates before (2019–2020) and during the pandemic (2019–2021). Changes in firearm death rates are further described by intent.
Results
Overall Firearm-Related Deaths
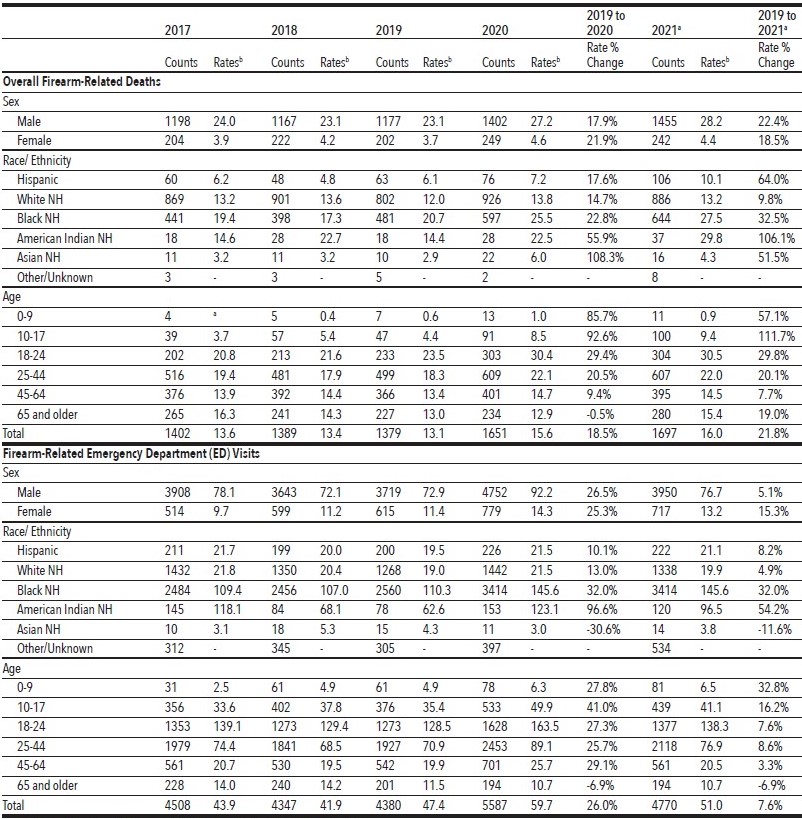
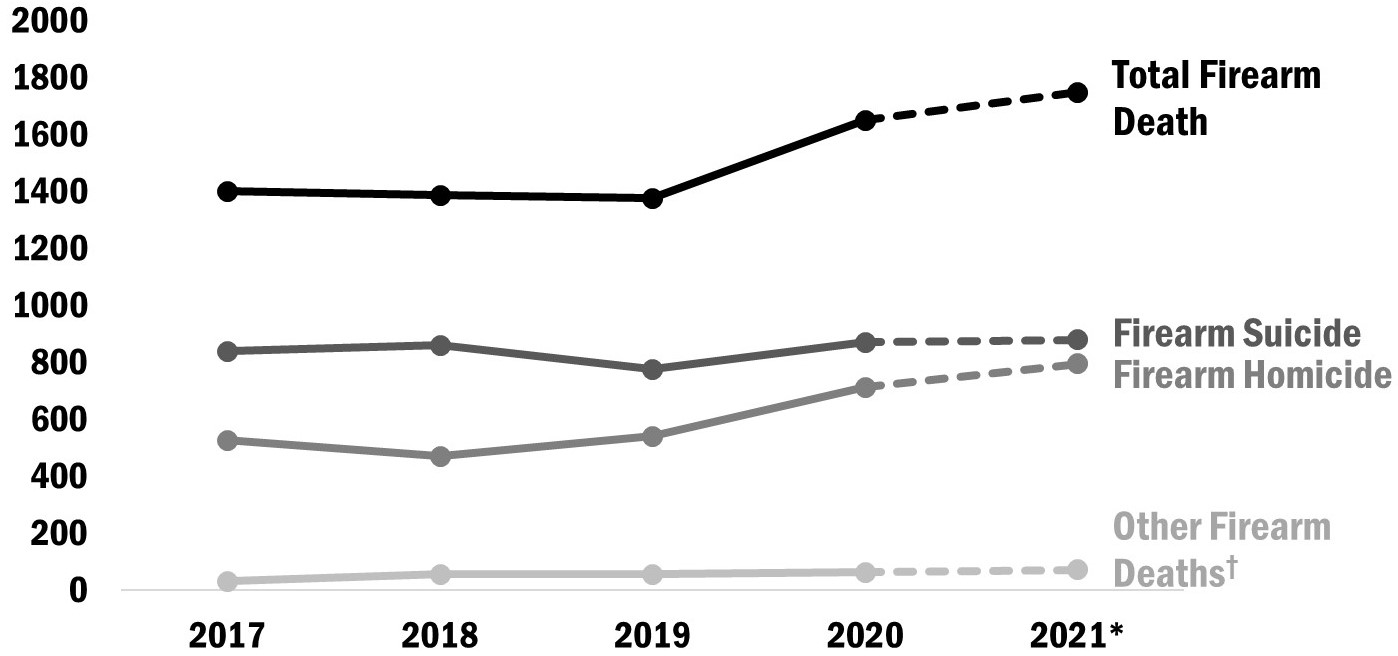
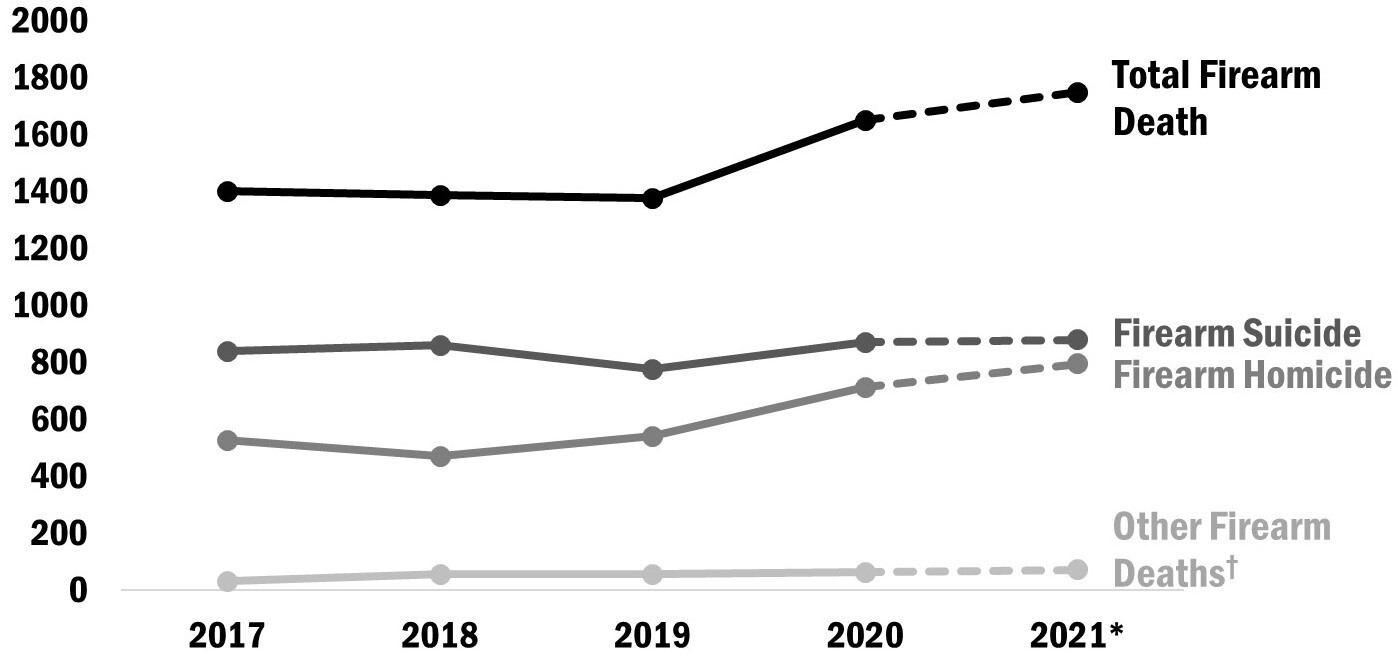
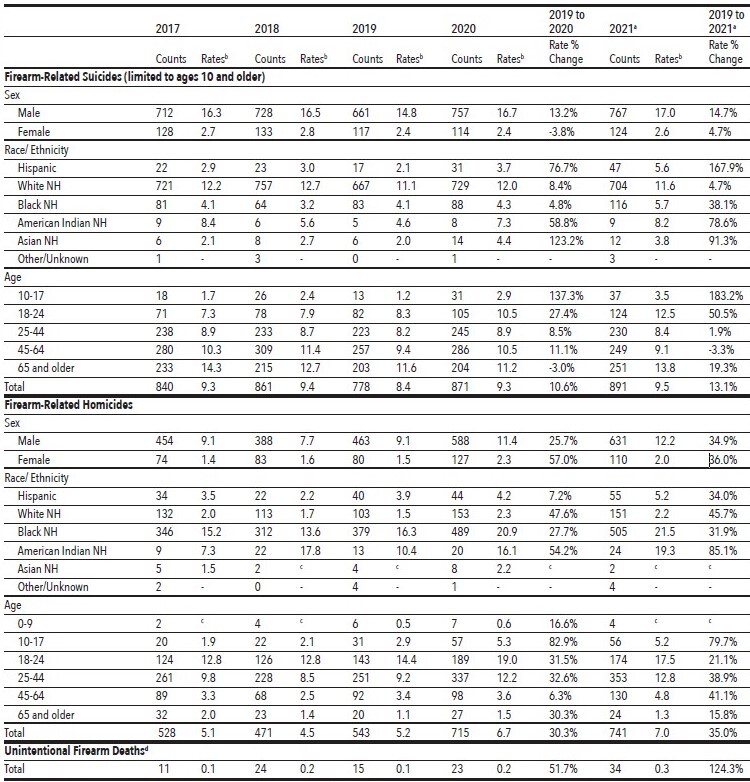
The number of firearm-related deaths increased by 19.7% from 2019 to 2020, and another 2.8% from 2020 to 2021 (N = 1379, 1651, and 1697 deaths, respectively; Table 1). Young adults aged 18–24 had the highest firearm-related death rate across all years, though the greatest increase during the pandemic years was observed among those aged 10–17 (111.7% from 2019 to 2021).
Firearm deaths continue to disproportionately impact Non-Hispanic (NH) American Indian and NH Black residents. Firearm death rates doubled among NH American Indians from 2019 to 2021 (14.4 to 29.8 per 100,000); rates also increased among Hispanic residents by 64.0% (6.1 to 10.1 per 100,000). NH Black residents experienced a 32.5% increase, and NH Asian residents a 51.5% increase from 2019 to 2021 (20.7 to 27.5 per 100,000 and 2.9 to 4.3 per 100,000, respectively; Table 1).
_visits__2017-2021_a_.jpg)
Firearm-Related Deaths by Intent
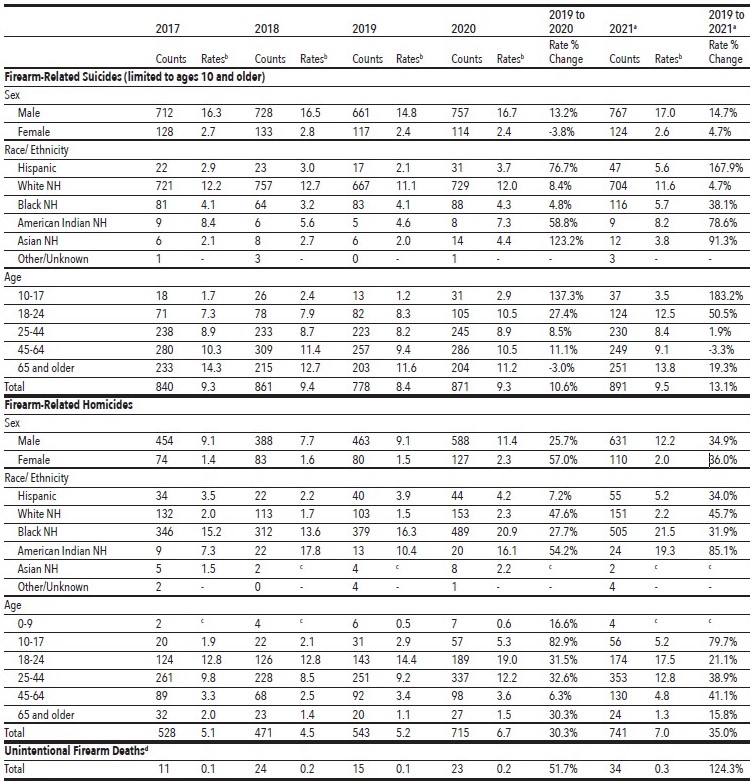
Changes in firearm-related death rates varied by intent. Unintentional firearm death rates increased 51.7% in 2020 and another 47.8% in 2021, while homicides increased 30.3% from 2019 to 2020 and 3.6% from 2020 to 2021. Firearm suicides increased 13.1% from 2019 to 2021. These differences varied further by demographic group. NH White victims continued to experience the highest firearm suicide rate in 2021 (11.6 per 100,000) yet had the lowest firearm suicide rate increase during the pandemic (4.7% from 2019 to 2021). Hispanic victims experienced the greatest firearm suicide rate increase from 2019 to 2021 (167.9%). Increases were also observed among NH Asian, NH American Indian, and NH Black victims (91.3%, 78.6%, and 38.1%, respectively; Table 2).
While firearm homicides increased across all racial and ethnic groups, NH American Indians had the largest increase in rates from 2019 to 2021 (85.1%; 10.4 and 19.3 per 100,000, respectively); rates remained highest for NH Black victims in 2021 (21.5 per 100,000). Despite persons aged 18–24 having the highest firearm homicide rate throughout the pandemic years (19.0 and 17.5 per 100,000 in 2020 and 2021, respectively), youth aged 10–17 experienced the largest increase from 2019 to 2021 (79.7%; 2.9 and 5.2 per 100,000, respectively; Table 2).
Firearm-Related Injury Emergency Department (ED) Visits
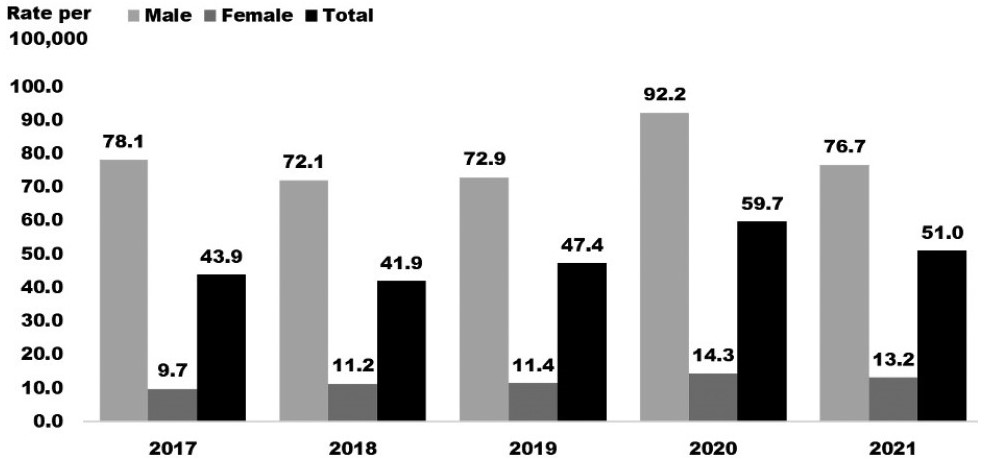
In addition to the spike in fatal firearm injuries, increases were also seen in firearm-related ED visits in North Carolina during the pandemic. Firearm-related ED visit rates increased 26.0% from 2019 to 2020 and 7.6% between 2019 and 2021 despite an overall decrease in ED utilization during this time period. Males have historically had much higher rates of firearm-related ED visits than females (76.7 and 13.2 per 100,000 in 2021, respectively); however, females experienced larger increases during the pandemic years (15.3% versus 5.1% increase, 2019 compared to 2021; Figure 2). Children under age 10 were the only age group that saw an increase in firearm-related ED visits in both 2020 and 2021 and had the highest rate change (32.8% from 2019 to 2021). The rate for NH American Indian firearm-related ED visits doubled from 2019 to 2020 (96.6%), the largest increase among any racial/ethnic group. The second-highest increase occurred among NH Black residents (32.0%, 2019 compared to 2020; Table 1). NH Asian residents were the only racial/ethnic group to experience a decrease in firearm-related ED visit rates (-30.6%, 2019 compared to 2020; Table 1).

Discussion
The COVID-19 pandemic not only affected people’s physical, emotional, and mental health, but also may have impacted the increase in firearm injury and death in North Carolina. During the first year of the pandemic, North Carolina experienced an 18.2% decrease in the overall number of ED visits for any cause.11 Despite this reduction in ED utilization, there was a 27.6% increase in the number of firearm-related visits in 2020 (Table 1). Similar changes were observed in the number of firearm deaths (19.7% increase in 2020), with alarming increases among youth (Table 1). Known risk factors for violence were exacerbated during the pandemic, including social isolation, lack of community support, economic stress, and media depictions of violence.1,2 Social inequities among communities were amplified, resulting in disproportionate increases in both firearm-related deaths and ED visits among vulnerable and other historically marginalized populations (Table 1).4 Generations of social, economic, and environmental inequities contribute to these disparities; it is crucial to recognize and acknowledge these systemic, avoidable, and often unjust factors that contribute to firearm-related injury and death.
Prevention of firearm violence and misuse is vital to bettering the lives of North Carolinians. Firearm ownership is deeply embedded in the culture of North Carolina, with almost half (42.1%) of North Carolina adults reporting having a firearm in or around the home.12 With increases in firearm purchases during COVID-19, ensuring that firearms are safely stored and that those handling firearms have adequate training and knowledge of firearm safety becomes increasingly important to helping mitigate firearm injuries.9,13,14 Ideally, firearms should be stored securely, locked and unloaded, to prevent injury.
The 2021 North Carolina Behavioral Risk Surveillance Survey estimated that 45.4% of firearm owners store firearms loaded; among those who keep firearms loaded in their homes, 53.0% also store their firearms unlocked.12 Three out of four children who live in a household with a firearm know where it is stored, including those under age 10.15 Additionally, the 2021 North Carolina Youth Risk Behavioral Surveillance Survey estimated that 29.5% of high schoolers could acquire and be ready to fire a loaded firearm without a parent or other adult’s permission in less than an hour.16 Unauthorized youth access can have fatal consequences.13 Safely storing firearms prevents accidental injuries among children, gun theft, and other unauthorized access from individuals who may wish to cause harm. Nine out of 10 people who survive a suicide attempt do not go on to die by suicide.17 Safe firearm storage provides a barrier to access and life-saving time when someone is experiencing suicidal ideation.10,11
The North Carolina Department of Health and Human Services (NCDHHS) has taken a public health approach to reducing firearm violence and misuse.10 This approach uses data and implementation of multilayered, evidence-based strategies to reduce firearm injury. North Carolina has defined resources for firearm-injury prevention and is working to expand adoption of these strategies statewide.10 Efforts to improve availability and access to timely, local data through NC-FASTER, NC-VDRS, and other systems will be imperative in planning and evaluating prevention strategies aimed at addressing these increasing firearm injury trends.18,19
Acknowledgments
The authors acknowledge the North Carolina State Center for Health Statistics and the North Carolina Violent Death Reporting System team for their work processing death certificates, law enforcement reports, and Office of the Chief Medical Examiner reports in order to provide quality data to use in injury and violence surveillance reporting.
NC DETECT is a statewide public health syndromic surveillance system, funded by the North Carolina Division of Public Health (NCDPH) Federal Public Health Emergency Preparedness Grant and managed through collaboration between NCDPH and the UNC-Chapel Hill Department of Emergency Medicine’s Carolina Center for Health Informatics. The NC DETECT Data Oversight Committee does not take responsibility for the scientific validity or accuracy of methodology, results, statistical analyses, or conclusions presented.
Disclosure of interests
For Lautenschlager, this report was supported in part by an agreement to the Council of State and Territorial Epidemiologists Applied Epidemiology Fellowship Program, which is funded by the Centers for Disease Control and Prevention (CDC). Cooperative Agreement Number 1NU38OT000297-03-00.
For Geary and the Injury and Violence Prevention Branch, NCDPH, North Carolina Department of Health and Human Services (NCDHHS), receives support from the National Center for Injury Prevention and Control, CDC.
For Waller and the Carolina Center for Health Informatics, funding support includes contracts with the Injury and Violence Prevention Branch, NCDPH, NCDHHS.