Introduction
The dental health of Army Reserve Component (National Guard and Army Reserve) Soldiers plays an important role in their medical/dental readiness to respond when called to duty; according to unpublished data from Medical Readiness Reporting (MRR), a tool built into the electronic health record, 60.5% of these Soldiers deemed medically/dentally not ready to deploy are deficient in their dental requirement. Diagnosing and correcting dental conditions likely to require emergent care during a 12-month deployment (DRC 3 conditions) is an integral part of keeping a Soldier medically/dentally ready1 and requires both military and civilian dentists’ support. Reserve Component Soldiers are often required to respond on short notice, and late diagnosis of complex dental conditions can result in not being ready to deploy. Just-in-time treatment of dental issues taxes treatment capabilities and often interferes with training.2 Dental disease non-battle injuries (D-DNBIs) or dental emergencies have historically accounted for over 15% of all disease and non-battle injuries in a deployed environment.3 The D-DNBI rate was measured at 152/1,000 Army National Guard (ARNG) Soldiers and 184/1,000 Army Reserve Soldiers deployed annually to Iraq and Afghanistan between May 2009 and December 2012; approximately 20% of those D-DNBIs were severe enough to cause a limitation of operational capabilities.3 In a deployed environment where dental assets are limited, access to care is limited as well. Seeking dental treatment in a deployed environment becomes a logistical issue and is therefore best avoided. This article addresses successes in improving access to care for Reserve Component (RC) Soldiers using the military health system as well as opportunities for North Carolina civilian dentists to support the effort. To achieve health for RC Soldiers, it will take teamwork between the military and civilian dental teams.
Efforts Underway to Meet Soldiers’ Dental Requirements
Extensive efforts have been made to address the dental health and readiness of our RC Soldiers. Prior to 2009, dental treatment to correct deployment-limiting dental conditions was not funded by the military unless the Soldier was alerted for deployment. Implemented in fiscal year 2009, the Army Selected Reserves Dental Readiness System (ASDRS) and associated Reserve Health Readiness Program (RHRP) fund treatment of deployment-limiting dental conditions for non-alerted RC Soldiers at no cost to the Soldiers. ASDRS does not provide dental insurance, but rather dental treatment as part of readiness operations. ASDRS also does not fund routine or preventive care; it is limited to treating more advanced deployment-limiting conditions.4
Historically, achieving dental readiness in the RC has been challenging. From 1990 to 2008, Army Reserve Component dental readiness remained below 50%.4 By 2012, after just three years of funding dental treatment of non-alerted Soldiers to correct DRC 3 conditions, baseline dental readiness had improved to 81% (unpublished data, MEDCHART MRR, 2012). In January 2020, prior to disruptions in readiness operations due to the COVID-19 pandemic, baseline dental readiness among ARNG stood at 94.1%, just shy of the Army’s 95% dental readiness goal.5 In June 2023, ARNG dental readiness stood at 89.3% and Army Reserve dental readiness at 81.6% as we work to regain pre-COVID-19 levels.4
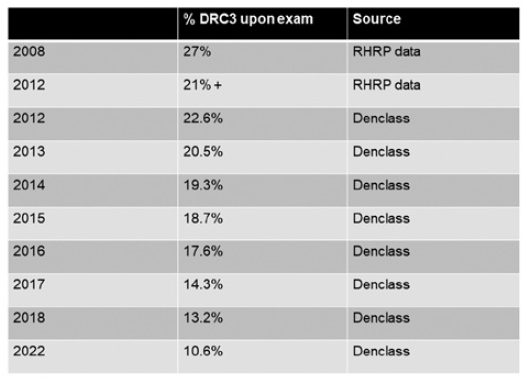
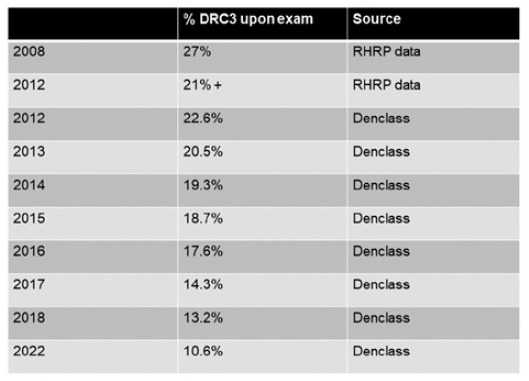
Looking at another metric, in 2008, pre-ASDRS, 27% of Soldiers were found to have deployment-limiting (DRC 3) dental conditions upon exam; by 2012, after funding dental treatment for non-alerted Soldiers for three years, that number had dropped to 21%.4 The DRC 3 rate upon exam has continued to improve every year and stood at 10.6% ARNG in fiscal year 2022 (Figure 1). Funding for dental treatment has resulted in great improvement in readiness metrics, reflecting a dentally healthier and readier force.
RC Soldiers have multiple pathways available for meeting dental readiness requirements. Soldiers receive dental exams every 12–15 months as part of readiness operations, and treatment to cure DRC 3 conditions identified at these exams is often available through contracted providers at the time of diagnosis. The Limited Dental Treatment Program (LDTP), a recent ARNG initiative, expands the role of commissioned Dental Officers to be direct providers of dental treatment for Soldiers who are in drill status. If a deployment-limiting condition is not cured at mission, it can be treated though the RHRP voucher program, which funds required treatment at participating civilian community dental providers. The RHRP voucher program is limited to treating more advanced deployment-limiting conditions; it does not fund routine and preventive care. Recent initiatives aim to open dental treatment facilities (DTFs) across the military service spectrum to support Army Reserve Component dental readiness requirements,5 however, such support may be constrained by limited treatment capacity. Soldiers have the option of receiving self-funded, private-sector care and submitting a form (DD 2813) signed by their private dentist updating their dental readiness status. Identifying private practice patients as RC Soldiers by adding a question to the health history form may be helpful in facilitating completion of the DD 2813 form. It is essential for private dentists performing dental examinations on Soldiers to be educated on the Army Dental Readiness Classifications and calibrated in their assessments to ensure accurate readiness reporting.
Insurance Options
Drilling RC Soldiers who are not on full-time orders can purchase the TriCare Dental Program (TDP), which partially covers access to private-sector dental care, either as an individual policy or for their family. The cost of TDP is partially subsidized, but there is a monthly fee as well as a deductible, copay, and maximum yearly benefit for all services beyond preventive. According to the Surgeon General, only 12% of drilling Soldiers enroll in the TriCare Dental Plan (Kiersey G. “Overview and Assessment of Army National Guard [ARNG] and U.S. Army Reserve [USAR] Access to Dental Care to Support Total Army Readiness,” 2019, unpublished).
Full-time Active Guard Reserve (AGR), Active-Duty Operational Support (ADOS), and deployed and alerted Soldiers currently have TriCare Prime dental insurance and are expected to get most of their dental care from a military DTF. If residing more than 50 miles from a DTF, these Soldiers may opt for care through the Active-Duty Dental Program (ADDP), which accommodates civilian care from participating providers. DTFs may delegate care to ADDP as required.
House Resolution 8113, the Dental Care for Our Troops Act, sponsored by Representative Andy Kim (New Jersey) and currently referred to the House Committee on Armed Services, would waive premiums and copays for the TriCare Dental Program, providing all RC Soldiers with dental insurance that covers routine and preventive care as well restorative procedures.6 The bill also provides access to private-sector dental care. Adoption of HR 8113 would be a big step forward for the health and readiness of our Soldiers.
Conclusion
Huge advances in dental readiness have been achieved since dental treatment to cure DRC 3 conditions for non-alerted Soldiers was funded in 2009. Still, a DRC 3 rate of greater than 10% upon exam and a baseline dental readiness of under 90% leave room for improvement. Baseline dental readiness continues to fall short of the Army’s 95% dental readiness goal. Private-sector dentists can be part of the solution by participating in the TriCare Dental Plan and Active Duty Dental Plan via www.uccitdp.com, and can learn about insurance options available to our Soldiers and the RHRP voucher program at www.qtcm.com. Dental insurance at no cost to the Soldier that provides access to routine, preventive, and restorative care in the private sector as proposed in HR 8113 may be the next big step forward.
Disclosure of interests
This article was reviewed by Army National Guard Public Affairs and OPSEC. No interests were disclosed.