During the COVID-19 public health emergency (PHE), NC Medicaid allowed approved hospital facilities or systems to provide acute hospital care at home.1 Originally a program designed for the Medicare population, offering coverage of care provision for significant illness outside of traditional inpatient settings is one example of how Medicaid programs across the country rapidly evolved to meet the challenges of the pandemic. Historically, transitioning to new models can take public payors many years for public to adopt. Previous studies examining outcomes for populations cared for using a “Hospital at Home” (HaH) model have shown either favorable results or no significant differences in readmission rates, length of stay, and emergency department (ED) visits as compared with populations served by traditional inpatient hospitalization.2–6 To guide policy planning, NC Medicaid partnered with an external quality review organization, Health Services Advisory Group, to examine whether these outcomes were consistent among beneficiaries receiving HaH services.
The analysis compared 240 NC Medicaid HaH claims (associated with 234 beneficiaries) from March 2021 to August 2022 with a comparison group of 240 NC Medicaid claims for traditional inpatient hospitalization. The groups were matched on beneficiary age, gender, race, ethnicity, COVID-19 diagnosis, and Chronic Illness and Disability Payment System risk model score using propensity score matching. Measures included average length of stay (LOS), all-cause 30-day readmission, ED visit within 30 days after discharge, and primary care provider (PCP) follow-up visit within 30 days after discharge. Measure data sources included both administrative (final adjudicated paid claims) as well as ancillary data sources (identifiers associated with claims hospitals reported as being for HaH services). For the HaH group, over 94% of the ancillary data sources identified claims from a single hospital system. The comparison group included inpatient claims from the same hospital systems, with similar diagnosis codes found in the HaH claims.
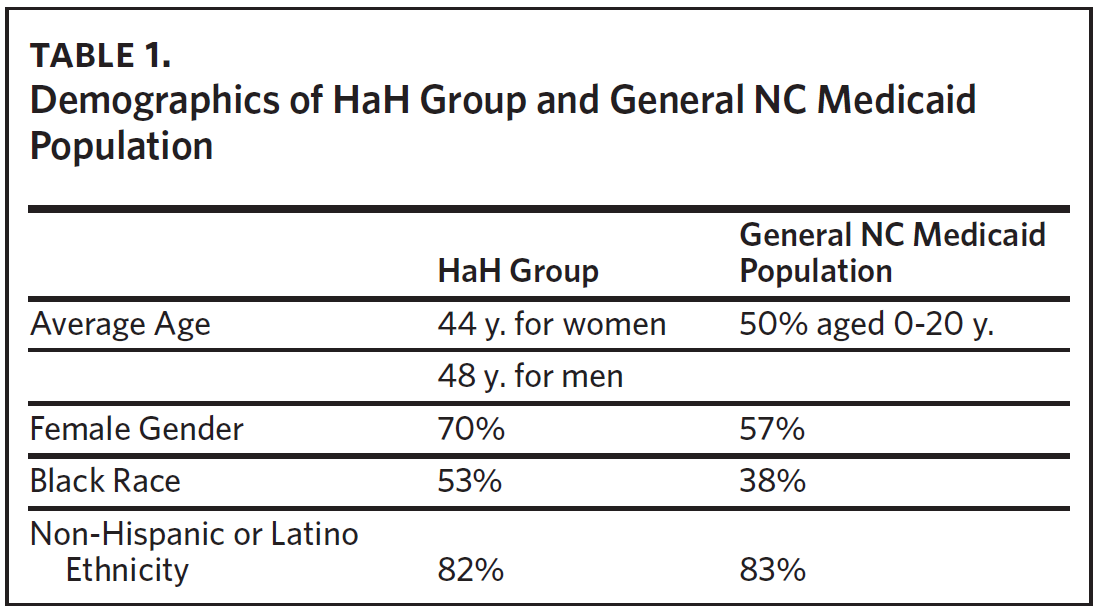
Demographics of the HaH group reflected 70% women with an average age of 44 years, while the average age for men was 48 years; 53% of the HaH cohort identified as Black, 42% White, and 82% non-Hispanic or Latino. The sample had more women and Black participants than the general NC Medicaid population, which is 57% women, 38% Black, 57% White, and 83% non-Hispanic or Latino. Half of the general NC Medicaid population is aged less than 21 years (Table 1).

As compared with the matched cohort, PCP follow-up visits within 30 days occurred at a significantly higher frequency in the HaH group (52.1% for HaH group versus 42.5% for comparison group). The small HaH population limited its statistical power to detect other significant differences, including ED visits within 30 days (13.8% for HaH group versus 8.3% for comparison group) and all-cause 30-day readmissions (12.9% for HaH group versus 10.0% for comparison group). Average LOS appeared similar for both groups (7.9 days for HaH, 8.2 days for comparison group).
In conclusion, as compared with the general NC Medicaid population, more women beneficiaries and Black beneficiaries were served by the HaH program as reflected by claims from predominately one hospital system during March 2021–August 2022. Compared with matched claims, the HaH group was significantly more likely to follow up with their PCP. Average LOS for both groups was approximately eight days. Small sample sizes limited statistical power; no significant difference was seen in other metrics.
Discussion
As compared with previous HaH studies looking at populations other than Medicaid beneficiaries, these results appear less favorable overall. Although beneficiaries participating in HaH were significantly more likely to follow up with their PCP, it is not clear whether patients in this cohort were motivated to see their PCP due to improved symptoms and/or desire to be compliant, or due to lack of symptom resolution or worsening symptoms. Higher (although not statistically significant) percentages of ED visits and all-cause readmissions in the HaH group may support the theory that PCP visits occurred more frequently in this group due to the latter. Patients receiving HaH supports in this analysis were approximately 30 years younger than those in another study examining outcomes among HaH participants in a Medicare/private insurance population,4 so the less favorable results are particularly surprising. One might expect that people who are healthier overall might be selected for HaH as compared with inpatient care. If studies involving older people (who generally are less healthy than younger people) demonstrate more favorable or neutral outcomes on ED follow-up and readmissions with HaH care, younger individuals might be expected to have even more favorable outcomes. Instead, these data suggest the opposite.
Medicaid is a safety-net program offering health care benefits to vulnerable populations. The majority of individuals are eligible for Medicaid benefits due to low income. Low-income individuals, by definition, have fewer financial resources. This often translates into fewer social resources, reduced housing quality and stability, and reduced access to health-related resource needs (such as healthy food, ready transportation, and safe communities). These factors may contribute to the less favorable results for Medicaid HaH participants as compared with HaH participants covered by Medicare or commercial insurance. If Medicaid is a proxy for generally lower income and less access to other supports needed to promote recovery from illness, it is possible that this population may benefit from traditional inpatient hospitalization more than those covered by other insurance products. Perhaps time spent in a safe hospital setting with easy access to meals and social support provided by clinical care team members offers Medicaid beneficiaries in particular a distinct advantage in promoting recovery from illness.
NC Medicaid and other state Medicaid programs began to offer coverage for HaH services during the COVID-19 pandemic, when there was a real and immediate need to free up hospital beds for patients requiring inpatient care and monitoring. Many states stood up field hospitals at some point during the PHE in response to overwhelming numbers of people with severe symptoms from COVID-19 infection. Clinical care team members were spread exceptionally thin and the physical and emotional demands on this workforce were considerable. As the pandemic wore on, in addition to the demands of direct patient care, clinical care team members also were often lightning rods for patient and family member frustration and stress. This stress came from many sources: income disruption, limited social interactions, confusing (and sometimes conflicting) guidance from public health authorities, masking requirements, and concerns about COVID-19 vaccine side effects. There also was significant concern around viral contagion; early in the PHE, it was not clear how the virus spread, but one effective intervention for reducing viral transmission was physical distancing between people. The HaH program offered participating individuals greater physical distancing (reducing viral exposure in those with non-COVID-19 diagnoses and reducing transmission for those with COVID-19 diagnoses), reduced health care workforce burden, and increased hospital bed availability for severely ill patients.
It was also not clear why the distribution of women and Black beneficiaries in the HaH program differed from the distribution of women and Black beneficiaries in the overall Medicaid population. Possible explanations include perceived higher levels of compliance among women as compared with men, perhaps leading health care providers to consider women to be generally lower risk for this type of lower-touch care.7 Black beneficiaries may have been perceived to have greater available social supports than White beneficiaries, making them more appropriate for this model of care.8 Conversely, higher numbers of Black beneficiaries and women beneficiaries in the HaH group may also reflect a pattern of race and gender bias, where White beneficiaries and male beneficiaries were prioritized to receive the more resource-intensive intervention of traditional inpatient care. For the future, it may be informative to look at the proportion of women and Black beneficiaries in the HaH program in the context of the population of patients with an inpatient admission and overall population or catchment area served by specific hospital systems.
The analysis described in this article does not provide insight into how beneficiaries were identified to receive care through the HaH model versus traditional inpatient care. Presumably, with matched diagnoses and chronic disease states, these factors played less of a role. It is possible that the factors that led clinical care teams to recommend HaH for one person and traditional inpatient care for another were influenced by unconscious bias. Future studies examining criteria used by clinical care teams to identify subpopulations of Medicaid beneficiaries for whom HaH care is appropriate would be valuable. These criteria ideally would include not only clinical elements, but also specific social and demographic factors that might influence decision-making. A HaH model shifts a significant portion of the caregiving responsibility to family members or friends, and this burden must be acknowledged. Longer term, clear, evidence-based selection factors linked to favorable outcomes for the HaH model are needed. The need for such criteria in the Medicaid population appears particularly apparent, given the limited research on use of this model in this unique and financially vulnerable population.
This analysis is limited by its relatively small sample size, as well as its focus on administrative data. Although such data are readily available to state Medicaid programs, administrative data often do not prioritize clinical accuracy. Diagnoses as reflected by ICD-10 codes, for instance, tell only a portion of a patient’s story. The nuances and complexity of patient care and factors contributing to selection of a HaH model of care over inpatient care delivery for an individual patient, or reasons for PCP follow-up visits within 30 days after discharge, are often not reflected in administrative data. For example, smoking history recorded within an electronic health record may factor into clinical decision-making about the appropriateness of HaH care but not be reflected consistently in administrative data. The analysis is also limited by its data from predominately one hospital system. It is not clear whether other systems would provide HaH services in a manner that would improve outcomes for this population.
After extensive study, review, and stakeholder discussions, NC Medicaid made the decision to cover HaH until December 31, 2024, when the Center for Medicare & Medicaid Services (CMS) waiver flexibility is scheduled to end. The program is currently pursuing a follow-up analysis with improved identification of HaH claims (ancillary data are no longer required to facilitate claims identification). There is particular interest among NC Medicaid leadership in examining whether HaH programs delivered during or after the PHE, such as NC Medicaid’s, relied more on virtual monitoring of HaH patients as compared with earlier programs with superior outcomes. As the model matures with more experience and more health systems participating, it is the expectation that outcomes should improve to meet those seen in other studies.
Conclusion
Providing HaH coverage during the pandemic offered advantages of greater physical distancing for HaH participants and freed up hospital beds and hospital care team members to serve severely ill patients. Coverage for such services also reflected the changing landscape of Medicaid programming. While not overwhelming, early evidence seems to suggest that as compared with people covered by Medicare or commercial insurance, the Medicaid population may benefit more from traditional inpatient care over HaH care, despite being decades younger on average than the Medicare population. Very low-income individuals, such as those qualifying for Medicaid benefits due to income eligibility, may have limited at-home supports needed to promote recovery from serious illnesses. Suggested areas of future study include evidence-based selection criteria for HaH care for Medicaid members, examination of HaH outcomes across different hospital systems, and possibly examination of the impact of provision of non-medical but health-related resources (such as healthy food) on outcomes for HaH participants. As additional research is done in this area, the program will continue to assess its value for beneficiaries.
Acknowledgments
A manuscript describing the results of this evaluation has also been submitted to JAMA Open.
Conflicts of interest
The authors have no potential conflicts of interest to acknowledge.