Introduction
Transgender and gender diverse (TGD) persons face significant social,1–3 economic,2,3 and health disparities.2–5 The 2022 U.S. Transgender Survey identified heightened health care concerns (e.g., avoidance of doctors due to fear of mistreatment) and negative health care experiences related to gender identity.6 Crucially, gender affirmation through transitioning, use of hormone therapy, and/or use of surgery was associated with higher life satisfaction among respondents.6
Compared to the rest of the United States, North Carolina was recently estimated to have the highest rate of transgender adults aged 18 and older at 0.87% and a moderately high rate of transgender youth aged 13–17 at 1.27%.7 At the same time, the 2022 U.S. Transgender Survey listed North Carolina among the top ten states that TGD persons have left due to laws targeting transgender persons.6 Among the many proposed anti-trans bills in North Carolina in the past few years, a ban on initiating gender-affirming care for minors (including puberty-delaying medication, hormone therapy, and surgery) was passed into law.8
Political and other types of structural discrimination create barriers to health care for TGD patients.4,9 Negative health care experiences,2,3,5 physician bias,9–11 lack of adequate medical training,9,12,13 and inconsistency in applying medical protocols10,14 have been identified as some of the physician-related barriers to care within the health care system. While health care experiences of TGD persons in the southern US have been examined,2,4,5 only a few small studies in this region have focused on physician factors.10,14 Family physicians are critical providers of TGD care due to their unique position in primary care, seeing patients across the lifespan (childhood through puberty, to adulthood and older age) with a lens oriented to family dynamics and comprehensive care.15,16
This study aimed to explore the factors that characterize family physicians who provide primary care (including chronic disease management and age-/organ-appropriate preventive screens) and/or gender-affirming care (GAC, primarily the use of medications to align natal sex characteristics with one’s gender identity) to TGD patients. We specifically sought to describe family physicians’ scope of practice and training experiences. Further, we aimed to identify personal and practice characteristics associated with the provision of TGD care among family physicians in North Carolina.
Methods
Study Development
The study was informed by a focus group of 7 individuals who either work closely with and/or personally identify as members of the TGD community in Southeastern North Carolina. Focus group activities were reviewed by the Novant Health Institutional Review Board (IRB) and deemed to be considered quality improvement and thus exempt. Focus group activities were completed in May 2022. The group offered suggestions about research project design and survey content. Informed consent was not collected from focus group participants, as these activities were not considered human subjects research by the Novant Health IRB.
Study Design and Survey
Using input from the focus group, the study team developed an observational study conducted via Qualtrics. The survey incorporated questions about physician practice for TGD patients generated by advisory group input and the authors’ clinical experience. The survey tool was also informed by the recommendation of Veale and colleagues17 to broaden TGD gender affirmation research to include sexuality, fertility/reproductive needs, routine health care, and non-medical health needs. Authors utilized the National Institute on Minority Health and Health Disparities Research Framework18 to ensure the project design touched upon multiple levels and domains of influence through specific survey questions.
The survey assessed several key physician characteristics, including demographics (e.g., age, race, political affiliation), scope of practice (primary care and/or GAC for TGD patients, reasons for not providing this care, perceived barriers to care for TGD patients), types of training in care for TGD patients, and clinic characteristics (e.g., payor types accepted, methods of advertising TGD care). Zip codes of residence and practice were included in the survey to allow for county-level comparisons across the state, using both US Department of Agriculture Rural-Urban Continuum codes19 and NC Medicaid Managed Care region designations.20 In analyses regarding Medicaid Managed Care regions, region 6 was used as the area of reference due to the high concentration of health risk factors and worse health outcomes in this area, particularly in the counties just inland to the coast.21 The 3 key outcome variables of interest were categorical and included: participation in TGD training (“Have you participated in any type of education or training in TGD patient care?”), providing TGD primary care (“Do you personally provide primary care [including chronic disease management and/or age-and organ-appropriate preventive screens] to TGD patients?”), and providing GAC to TGD patients (“Do you personally provide gender-affirming care to TGD patients?”). A full copy of the survey with all questions is available in Appendix A.
Participants and Survey Administration
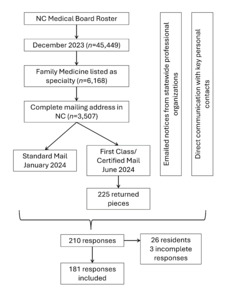
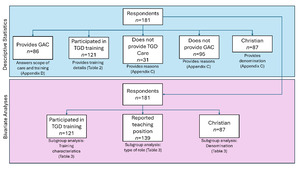
Any licensed family physician who practices in North Carolina and who also completed residency training (i.e., attending) or family medicine resident in North Carolina who was in their third year of residency training (nearing completion of training) was eligible to participate. The study was open from January 21, 2024, through September 30, 2024. The survey link and QR code were distributed via mailed postcard advertisements in two separate mailings a few months apart to family physicians listed on the North Carolina Medical Board roster, via emailed notices from statewide professional organizations (the North Carolina Academy of Family Physicians and the North Carolina Medical Society), and by direct communication with authors’ personal contacts across the state (see Figure 1). This study was evaluated and determined exempt by the University of North Carolina at Chapel Hill (#23-0105) and Novant Health IRBs (#22-2185). Participants indicated consent electronically through the survey tool; a waiver of written consent was provided by both IRBs given the online nature of the study.
Partway through the study, bots accessed the study for gift card money. Thus, the electronic survey was closed for a 2.5-week period halfway through the study to address and remove bot-generated responses. Upon reopening the survey, participants were asked to email the research team to obtain the survey link and complete a newly implemented CAPTCHA.
Analysis
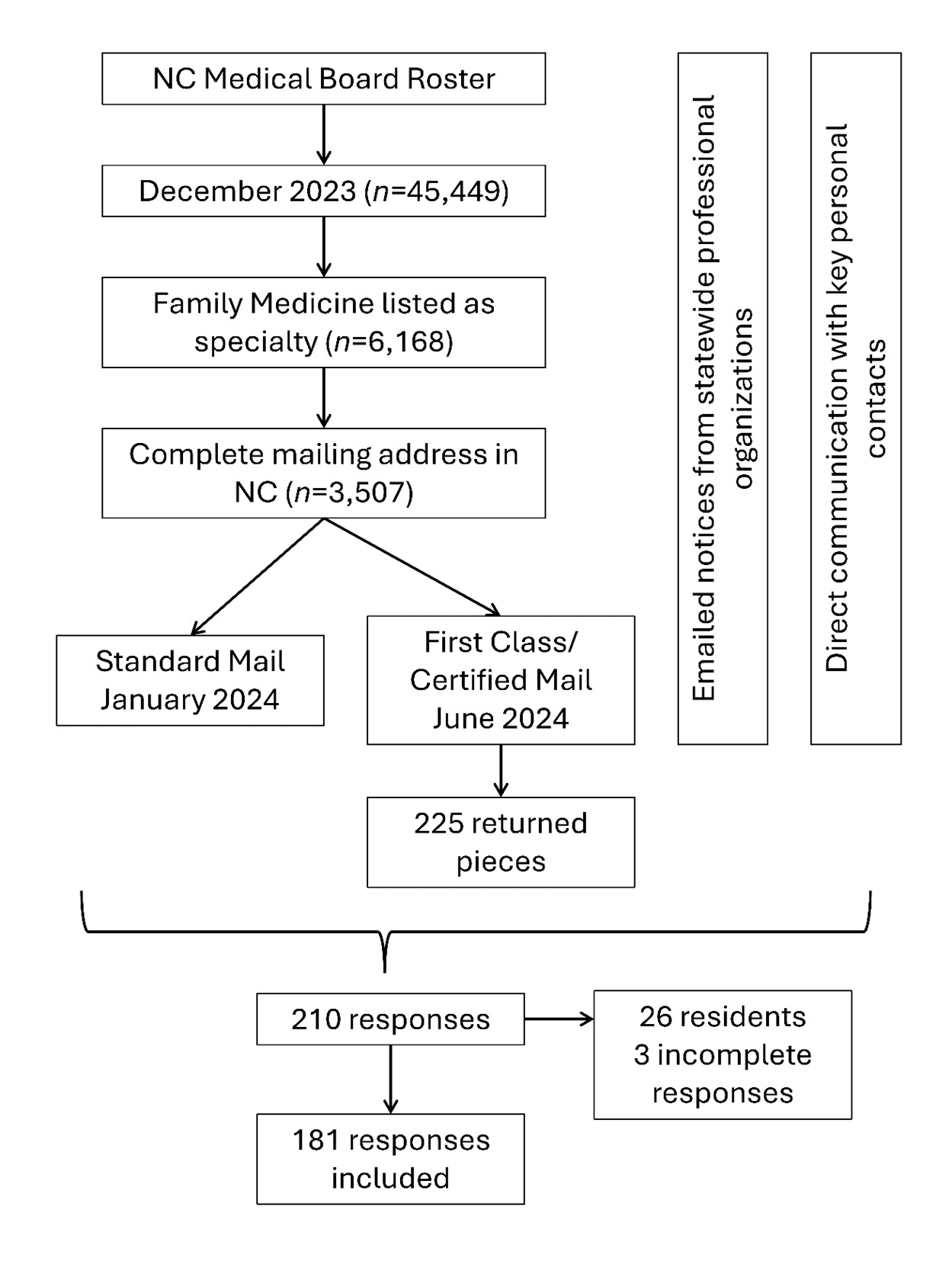
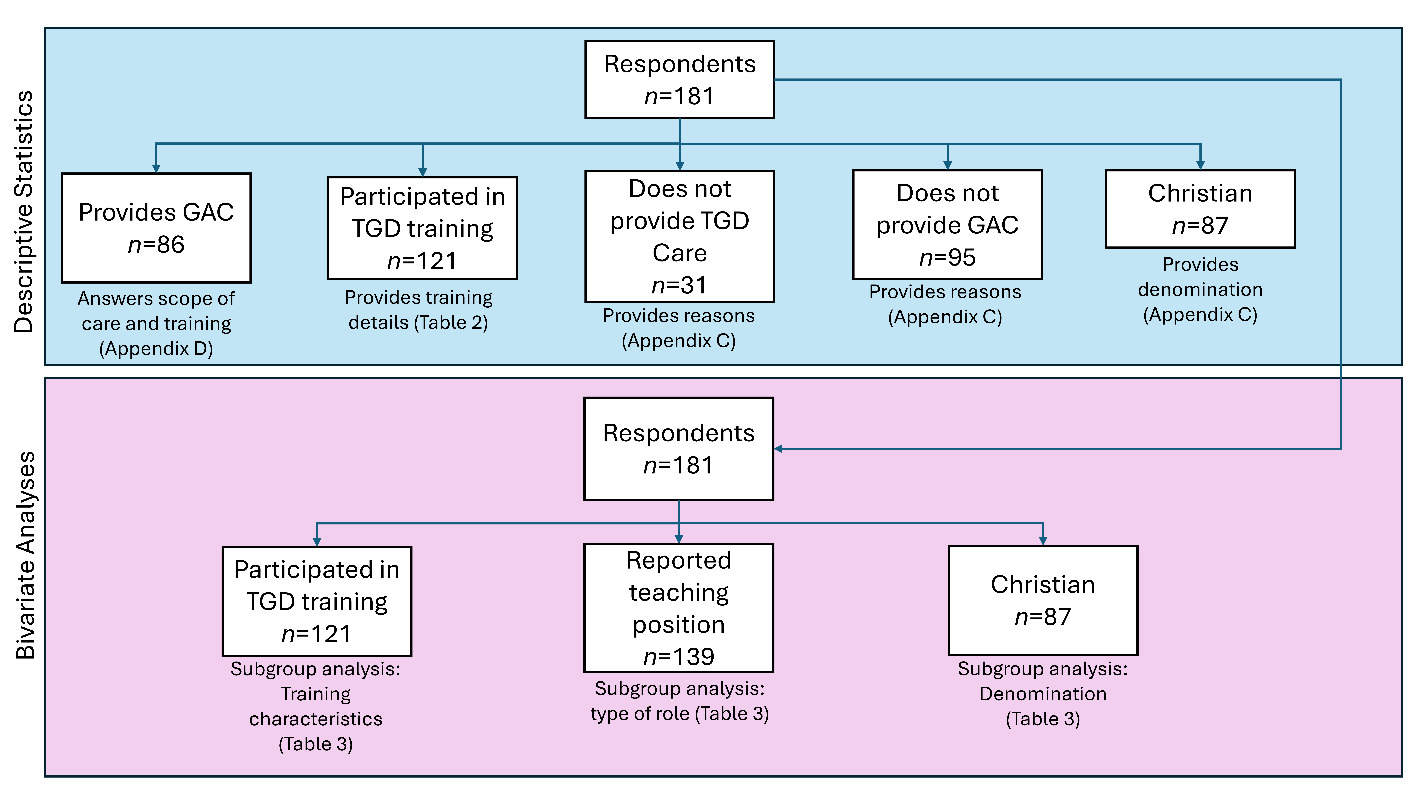
All statistics were conducted in R 4.2.1.22 Descriptive studies first utilized counts, means, and standard deviations to assess demographics and overall physician beliefs about and care practices for TGD patients; Figure 2 shows the subgroupings used for various analyses. Each of the 3 key outcomes—TGD training, TGD primary care, and GAC—were first assessed descriptively.
Next, bivariate analyses assessed factors associated with providing primary care and GAC to TGD patients. For continuous and ordinal variables, logistic regression was used to estimate associations with the provision of care and accompanying odds ratios. The association of categorical variables with the provision of care was assessed using Chi square analyses, or Fisher’s exact test if any cell had counts less than 5.23 If any cell was 0, a Haldane-Ascombe correction was applied.24,25 Odds ratios for categorical variables were calculated using the epitools package in R,26 with unconditional maximum likelihood estimation for Chi square tests and conditional maximum likelihood estimation for Fisher’s exact tests.27 For questions in which multiple responses could be selected, each response option was analyzed separately as a dichotomous variable (response selected/not selected). For each bivariate analysis, results were reported in the form of odds ratios, with 95% confidence intervals.
To control the false discovery rate given the large number of analyses, the Benjamini-Hochberg procedure was applied.27 For the Benjamini-Hochberg procedure, each family of tests was defined as all independent variables tested against a single dependent variable (Appendix B). Benjamini-Hochberg critical values were calculated with a false discovery rate of 5% (Q = .05), aligned with the alpha selected for this study. Pairwise deletion was used to manage missing data in bivariate analyses.
Results
Participants and Key Outcomes
Out of an estimated 3282 successfully mailed advertisements, 207 physicians completed the survey, making for a response rate of 6.4% (Figure 1). Of the 207 participants who completed the survey, 181 (87.4%) were attendings and 26 (12.6%) were third-year residents. Due to the low response rate from residents, only attendings were retained for the final sample. Sample characteristics are described in Table 1.
TGD Scope of Care
Out of 181 attendings who completed the survey, 150 (82.9%) provided primary care to TGD patients, and 86 (47.5%) provided GAC (Table 1). Among the 31 physicians who reported they did not provide primary care to TGD patients, the most frequently reported reason was not having TGD patients (n = 10; 32.3%). Among the 95 physicians who did not provide GAC, the most frequently reported reason was insufficient training (n = 50; 52.6%). Further reasons for not providing care to TGD patients are described in Appendix C. Among the 96 physicians who offered GAC, 76 (88.4%) offered gender-affirming hormone therapy, and 63 (73.3%) offered other medications that influenced hormones (e.g., progesterone, androgen blockers). Additional details regarding GAC providers’ scope of practice are available in Appendix D.
TGD Care Training Experiences
Out of 181 physicians, 121 (66.9%) reported having participated in training related to caring for TGD populations. The types of training cited varied widely, but most physicians reported that their training occurred after residency and that it was optional (Table 2). The training modalities most frequently reported by physicians included continuing medical education (CME) conferences that included a session on transgender health, training during residency, and independent study.
Factors Associated with TGD Scope of Care
TGD primary care. Physicians who identified as cisgender women were more likely than those who identified as cisgender men to provide TGD primary care (Table 3). Higher comfort levels in providing either TGD primary care or GAC and more positive beliefs about the appropriateness of family physicians providing TGD or GAC were each associated with a greater likelihood of providing primary care to TGD patients. Physicians who reported that their practice communicated or marketed TGD care via word of mouth were more likely to provide TGD primary care; those who reported they were not sure how their practice marketed TGD care were less likely to provide TGD primary care.
Having participated with any type of training related to TGD patient care was not associated with providing TGD primary care. However, among the 121 physicians who reported participating in some type of training related to TGD care, those who reported that they completed a training via independent study or CME conferences that offered a session on transgender health were more likely to offer TGD primary care. Five variables were significantly associated with the provision of TGD care in bivariate analyses, but not after implementing the Benjamini-Hochberg correction: educator role (e.g., core faculty, adjunct), whether practice locations have made efforts to be more inclusive to TGD patients, physician self-reported political alignment, participation in optional rather than mandatory TGD care trainings, and physician race.
Gender-Affirming Care (GAC). Among physicians, cisgender women were more likely than cisgender men to report providing GAC (Table 3). Physicians who described themselves as more liberal or less spiritual were more likely to provide GAC. Providers who reported their clinics explicitly asked patients for their pronouns or had made efforts to be more inclusive to TGD patients were more likely to provide GAC. Physicians who reported that their clinic marketed TGD care via word of mouth or in advertising materials that made note of non-discriminatory practice were more likely to offer GAC; those who reported that there was no mention of TGD care in advertising materials or that they were not sure how TGD care was communicated were less likely to provide GAC. Of note, physicians who reported that their practices do not restrict patients with Medicaid were less likely to provide GAC compared to those whose practices limited patients with Medicaid.
Physicians who had participated in education or training in TGD patient care were more likely to provide GAC than those who had not. Further, among the 121 physicians who had participated in training around TGD care, those who completed training via independent study were more likely to provide GAC. Three variables were significantly associated with the provision of GAC in bivariate analyses, but not after application of the Benjamini-Hochberg correction: physician sexual orientation, practice size, and the advertisement of practice TGD care readily and widely to the community.
Discussion
This study provides initial insight into the current state of family physician practice around TGD care, including scope of practice, experiences of training, and factors associated with physician provision of TGD care. The findings suggest that training in TGD care is a central element in providing primary care and GAC for TGD patients. Further, the data highlight physician, clinic, and training characteristics associated with providing TGD care, which may inform future interventions to engage more family physicians in this practice.
The present study established that most family physicians who have TGD patients in North Carolina are willing to offer primary care to TGD patients, in line with research from other geographic regions in the United States.11 While it is encouraging that most family physicians are willing to provide primary care to TGD patients, increasing the number of clinicians who offer routine care to all patients is essential to ensuring equitable access. Roughly half of all survey participants reported providing GAC to TGD patients. Yet, a recent study found that only 29% of graduating family medicine residents plan to continue GAC in their future careers,28 highlighting a need for increased support for GAC practice.
Prior research has established that rates of GAC offerings increase when sufficient support and training are available.29 In the present study, participating in any type of education or training in TGD patient care was associated with higher rates of providing GAC. Further, insufficient training was cited as the most common barrier for providing GAC and the second most common barrier for providing TGD primary care.
In this study, physicians who completed training via independent study were more likely to provide TGD primary care and GAC, while those who completed training at a CME conference with a session on TGD health were more likely to provide TGD primary care. Self-directed learning is associated with greater training effectiveness in medical education,30 and thus, providing greater access to self-directed trainings may increase rates of TGD care. Alternately, physicians who are motivated to provide TGD care may be more likely to seek out dedicated training. Among family physicians who did not provide GAC in the present study, 15.0% reported that providing care for TGD patients was against their personal beliefs. Previous research has found that exposure to transgender individuals is associated with physician willingness to provide routine primary care to TGD individuals,11 and intergroup contact is effective at promoting more tolerant attitudes toward LGBTQ patients.31 Thus, training curricula that include experiential learning and intergroup contact may address physician attitudes.
Physicians in practices where Medicaid patients were not restricted were less likely to provide GAC, which underscores concerns about access issues for patients without private insurance who are seeking GAC.32 While not significant after accounting for the Benjamini-Hochberg procedure, participants who offer GAC trended toward being more likely to work at larger clinics where there may be more appointment availability. Larger clinics may also have access to more training opportunities. Future research with larger samples should confirm if clinic size is related to the provision of GAC.
Limitations
The present study was limited by a small sample size, which hinders the robustness of statistical conclusions that can be drawn from bivariate analyses. There is a possibility of selection bias by which participants most interested in the topic of TGD care may have been more likely to respond to the survey postcards, particularly after the influx of bot responses and subsequent requirement for participants to email the investigators for the survey link. A second mailing aimed to reduce potential bias by reaching more family physicians across the state, but the concurrent use of personal contacts to advertise the survey likely further skewed participation by location or institution. Together, the small sample size and potential selection bias limits the generalizability of findings. Future research will be needed to confirm if the results in this study remain robust in other samples. Further, recent policy changes regarding care of TGD patient populations may impact physician behavior, and future research is needed to assess care in a rapidly changing political landscape. Ultimately, the incidence of North Carolina family physicians offering TGD primary care in the present study was similar to previous research,11 and the present findings are best positioned to offer an initial picture of family physicians most interested in TGD care.
Conclusions
This study provides insight into the state of TGD care in North Carolina, including scope of practice, training, and factors associated with family physicians’ provision of TGD care. Training may be a key opportunity to increase access to TGD care in family medicine, with the aim of reducing health disparities for TGD patients across the state and beyond.
Acknowledgments
The authors would like to acknowledge the contributions of Victoria Scott; Julie Titter, MS, ATC; and Bridgette Cline, MPH, for their work in coordinating the study.
Data from this study were briefly summarized at the Symposium for Health Equity Research in Southeastern North Carolina in Wilmington, NC (March 2025), as well as the GLMA’s Annual Conference on LGBTQ+ Health in Minneapolis, MN (October 2025).
Declaration of Interests
The authors have no interests to declare.
Financial Support
The project described was supported by the Research Advisory Council of Novant Health, Novant Health New Hanover Regional Medical Center, University of North Carolina Health Care System, and University of North Carolina at Chapel Hill School of Medicine through the Promoting Health Equity in Research in Southeastern NC award (grant HE0201). The content is solely the responsibility of the authors and does not necessarily reflect the official views of the granting organizations.
Correspondence
Address correspondence to Kiran McCloskey, PhD, Office of Health Equity & Community Health, Novant Health, 4000 Frontis Plaza Blvd, Winston-Salem, North Carolina, 27103 (KMcCloskey@novanthealth.org).