Introduction
Medicaid is the standard health plan offered to low-income adults, children, pregnant women, older adults, and individuals with disabilities.1 According to the North Carolina Department of Health and Human Services (NCDHHS), NC Medicaid covers most services, including in-network provider visits, emergency care, dental care, vision and hearing services, prescription drugs, maternity and postpartum care, hospital services, behavioral health, and preventive and wellness services. On December 1, 2023, Medicaid eligibility in North Carolina expanded to include adults aged 19 to 64 earning up to 138% of the federal poverty level, extending coverage to more than 450,000 residents by April 2024 and 650,000 residents as of April 2025.2,3 The expansion had a notable impact on rural counties, as 233,000 of the new beneficiaries resided in those communities.3
Evidence on the effects of Medicaid expansion on emergency department (ED) utilization in other states remains limited and largely heterogeneous. Several studies indicated Medicaid expansion primarily altered the payer composition of ED visits rather than substantially changing overall utilization. For example, Zhao and colleagues found the share of ED visits covered by Medicaid increased, whereas visits by uninsured and privately insured patients declined.4 Similarly, Moghtaderi and colleagues reported substantial rises in Medicaid-paid ED visits and corresponding falls in uninsured visits between 2013 and 2016 but observed no statistically significant change in total ED visit volume or admission rates.5 These findings suggest that expansion often reclassifies previously uninsured ED users into Medicaid coverage without necessarily increasing overall demand for emergency services.4,5 National analyses of low-income adults by Miller and Cameron also found that Medicaid expansion was not associated with significant changes in total ED utilization but was linked to reductions in visits related to barriers to outpatient care.6
However, other studies have examined the direct impact of Medicaid expansion on ED use and have found evidence of changes in utilization. Giannouchos and colleagues determined that the overall number of ED visits declined in expansion states relative to non-expansion states following implementation of the Affordable Care Act (ACA), with reductions concentrated among non-emergent and primary care-treatable visits.7 These results suggest that improved access to primary and preventive care may reduce reliance on ED services for less urgent health needs.7 Conversely, Finkelstein and colleagues’ analysis of the Oregon Medicaid expansion experiment indicates that ED utilization may increase in the short term among newly insured individuals, likely reflecting previously unmet health care needs and greater access to care.8
State-level policy design may further contribute to variation in ED use across studies. For example, North Carolina Medicaid provides access to emergency services with no cost sharing, while other states may impose copayments, coinsurance, deductibles, or other out-of-pocket requirements for Medicaid-covered services.1,9 Evidence from health maintenance organization (HMO) models as highlighted by Selby and Swain suggests that even small ED copayments may reduce utilization by essentially perpetuating cost barriers which discourage non-urgent visits and encourage patients to seek care in alternative settings.10
Taken together, these findings demonstrate that while Medicaid expansion consistently shifts the payer mix of ED visits by reducing the number of uninsured patients, its effects on overall ED utilization remain context dependent. Our cohort study evaluated the relationship between Medicaid expansion and total ED visit volume across all of North Carolina’s 100 counties. We hypothesized that an increase in Medicaid enrollment was associated with fewer total ED visits when accounting for population changes, hospital bed availability, county urban-rural classification, Federally Qualified Health Centers (FQHCs), and Medication Assistance Program (MAP) sites.
Methods
We conducted a county-level (n = 100), pre-post analysis comparing total ED visit volume in the year (12-month period) preceding expansion (December 2022 to November 2023) with the year following implementation (January 2024 to December 2024). December 2023 was excluded due to active enrollment (Appendix A).
The primary outcome was the change in county-level ED visits obtained from the North Carolina Disease Event Tracking and Epidemiologic Collection Tool (NC Detect ED), a state-developed service provided by the North Carolina Division of Public Health in collaboration with the University of North Carolina (UNC) School of Medicine (ncdetect.org).11 The independent variables were as follows, with sources in parentheses:
-
b1 = change in number of Medicaid beneficiaries per county (North Carolina Department of Health and Human Services [NCDHHS])
-
b2 = most recent number of MAP sites available per county (NCDHHS)
-
b3 = net population change per county between 2023 and 2024 (census.gov)
-
b4 = change in number of FQHCs between 2023 and 2025 (NCDHHS)
-
b5 = number of FQHCs in 2025 (NCDHHS)
-
b6 = number of hospital beds available per county as of 2025 (NCDHHS)
-
b7 = urban-rural designation in 2025 (NCDHHS), with urban counties coded as 0 and rural counties coded as 1.
The regression model was specified as:
ΔED Visits = a + b1(ΔMedicaid beneficiaries) + b2(ΔMAP sites) + b3(Δpopulation) + b4(ΔFQHCs) + b5(FQHCs in 2025) + b6(hospital beds in 2025) + b7(urban versus rural)
Multivariate linear regression was conducted using Statistical Package for the Social Sciences (SPSS) through the University of North Carolina (UNC) Virtual Lab with consultation from the UNC Odum Institute (Appendix B). Statistical significance was defined as P < .05.
Model Explanation
The change in the number of Medicaid beneficiaries per county serves as the main independent variable. Net population change and hospital beds available across counties both serve as control variables in this analysis. Medication assistance programs have been shown to reduce ED utilization. Burley and colleagues (2016) found that patients receiving coordinated prescription assistance experienced a 51% reduction in ED and hospital visits.12 Similarly, a 2023 analysis of patients with chronic obstructive pulmonary disease (COPD) who were enrolled in a 340B prescription assistance program reported a significant decline in ED visits and hospitalizations in the year after enrollment.13 Our model accounted for the total number of and change in FQHCs across counties because evidence from Massachusetts supported their role in reducing ED utilization, particularly for conditions treatable in primary care or non-emergent settings.14 Finally, this model also accounted for urban-rural designation considering rural counties experience higher ED utilization compared to urban counties.15,16
Results
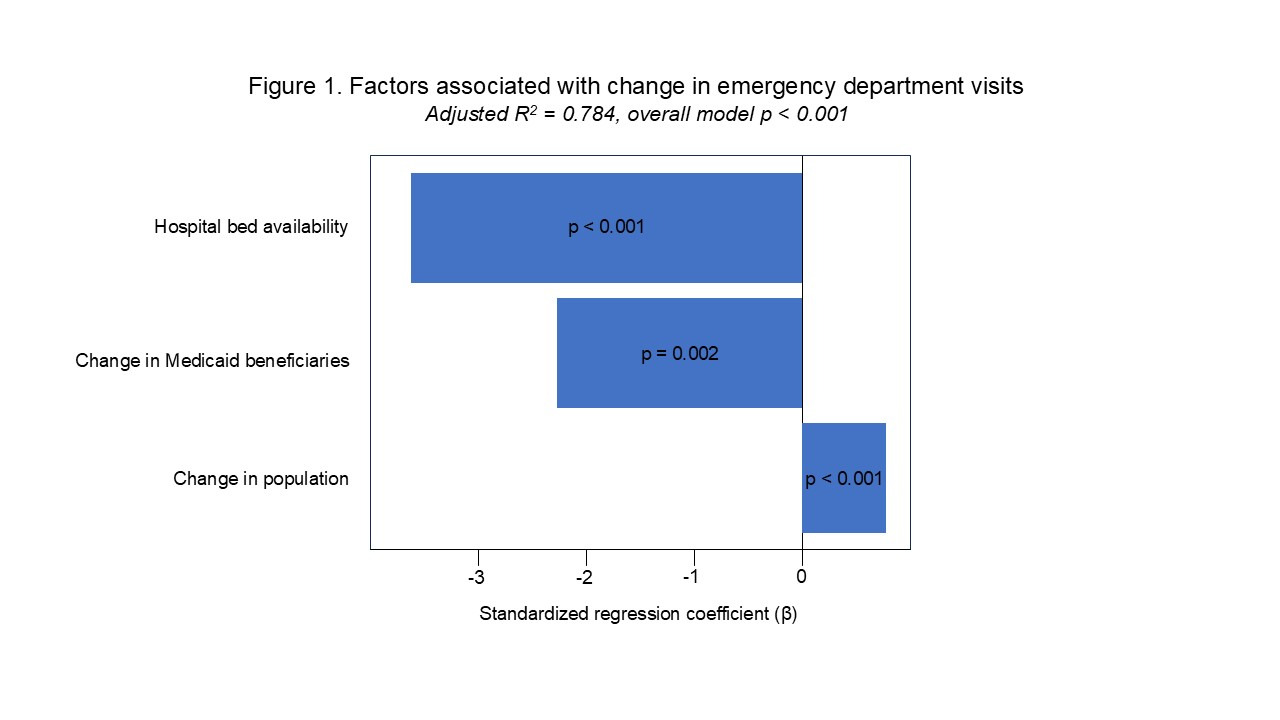
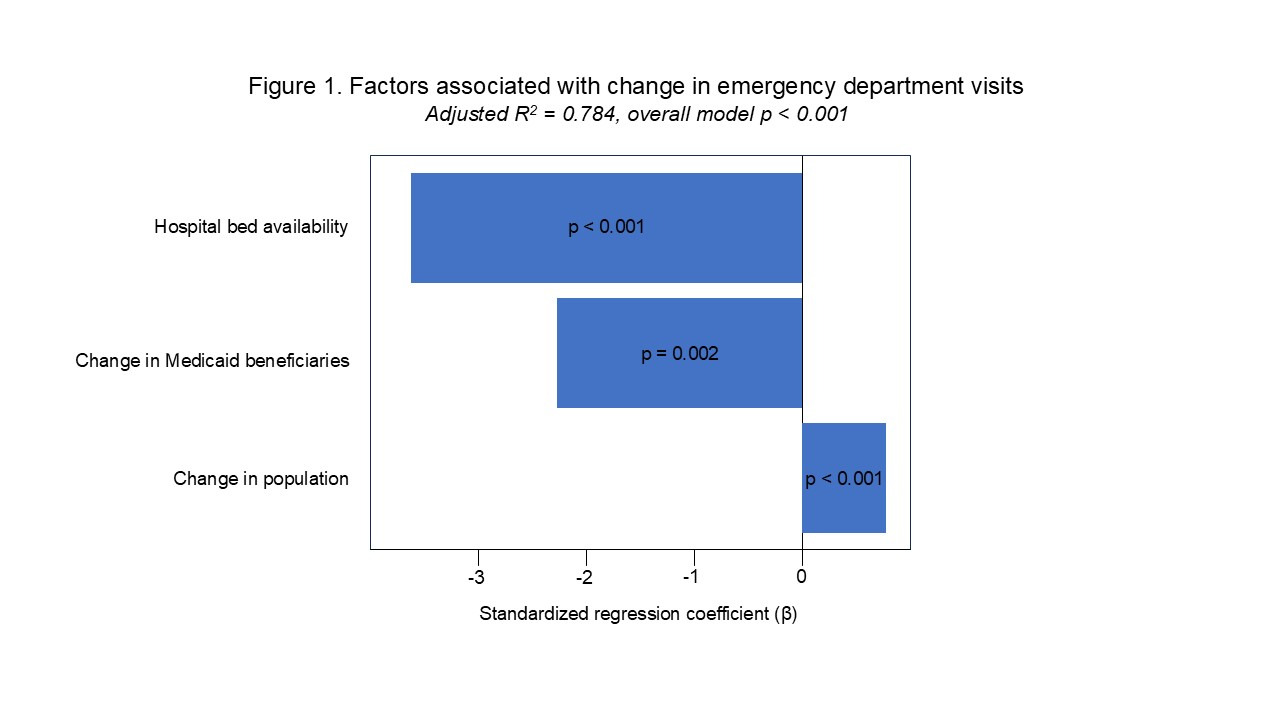
The model explained 78% of the variation in ED visits (adjusted R² = 0.784). ANOVA indicated overall model significance (F = 52.375, P < .001). Three variables were significantly associated with changes in ED visits (Figure 1). Population change demonstrated a positive association (standardized coefficient β = .756, P < .001). Hospital bed availability was inversely associated (β = −3.69, P < .001). Change in Medicaid beneficiaries was also inversely associated (β = −2.27, P = .002). Other variables, including change in FQHCs, absolute FQHC count, MAP distribution, and rural versus urban status, were not statistically significant. Correlations were notably observed between Medicaid beneficiary changes and population changes (r = 0.69, P < .001), hospital beds (r = 0.641, P < .001), and urban-rural county designation (r = −0.283, P = .004).
Discussion
Our county-level analysis suggests Medicaid expansion in North Carolina was associated with a reduction in ED visits one year after its enactment. This supports prior findings that expanded coverage may reduce reliance on emergency care.4 The mechanism behind the inverse relationship between hospital bed availability and ED visits remains unclear. One explanation is that greater bed capacity reduces pressure for early discharges, which may lower the risk of complications and subsequent ED readmissions. Another possibility is that increased bed availability allows for more direct admissions from outpatient settings and reduces the need for patients to enter through the ED, although this is anecdotally less common in practice.
The correlations reported in the results suggest that increases in Medicaid beneficiaries alongside growth in county population and the number of hospital beds are expected. As population size increases, the demand for health care services also rises, which may lead to a greater number of individuals qualifying for Medicaid. Similarly, counties with more hospital beds often have greater health care capacity, which is commonly associated with population growth and higher Medicaid enrollment. Finally, the correlation observed between Medicaid beneficiary changes and urban-rural county designation indicates that rural counties in North Carolina were more likely to experience increases in Medicaid beneficiaries compared to urban counties. These findings are consistent with prior evidence from the Kaiser Family Foundation, which reported that rural counties had a higher reliance on Medicaid.17
Our findings have important implications for health care administrators and policymakers, particularly in the context of the One Big Beautiful Bill Act of 2025 (House Resolution [HR] 1/OBBBA) which is expected to tighten Medicaid eligibility criteria in North Carolina over time. The potential rollback of Medicaid expansion could shift the ED payer mix toward a higher proportion of uninsured patients, thereby increasing uncompensated care costs for health systems statewide. Future research that estimates the cost savings associated with reduced ED utilization could provide valuable evidence to guide and justify state-level funding decisions regarding Medicaid expansion.
Our study’s limitations include reliance on county-level aggregate data, potential confounding from unmeasured health system changes, and the relatively short post-expansion observation window. It is important to note that Medicaid enrollment is highly dynamic. The number of beneficiaries continued to rise after December 2024, reaching about 650,000 by April 2025. We elected not to extend the study window beyond 12 months, since doing so could introduce additional confounders, including overlap with the pandemic-era period prior to December 2022 and potential shifts in ED utilization related to the pandemic. Finally, variables that were not found significant in the model may require an extended observation period to draw robust conclusions. Future research is needed to examine longer-term effects and determine other potential contributing factors.
Conclusion
North Carolina Medicaid expansion was linked to fewer county-level ED visits within one year, suggesting that broader Medicaid eligibility and coverage can help alleviate ED demand. These findings are particularly relevant after the passage of the One Big Beautiful Bill Act of 2025 (HR 1/OBBBA) which is expected to tighten Medicaid eligibility. Such changes could increase the proportion of uninsured patients and raise uncompensated care costs for hospitals. Future research estimating cost savings from reduced ED utilization can help inform state-level decisions on Medicaid funding and expansion.
Data Sharing Statement
The data used and referenced in this manuscript will be made available as supplemental files submitted with the manuscript. The supplemental materials include multiple spreadsheets representing different variables, a cumulative dataset formatted for use in the Statistical Package for the Social Sciences (SPSS), and the SPSS output file generated during the analysis. All data were collected from publicly available sources and will be accessible to readers upon publication. No additional restrictions or conditions apply.
Author Contributions
Drs. Gupta, Berner, and Ilaiwy had full access to the data and take responsibility for the integrity of the data and the accuracy of the analysis.
Concept and design: Gupta, Ilaiwy.
Acquisition of data: Gupta, Ilaiwy.
Statistical Analysis: Berner, Ilaiwy, Gupta.
Drafting of the letter: Gupta, Ilaiwy.
Critical Review of the Manuscript: Ilaiwy, Berner.
Supervision: Ilaiwy.
Declaration of Interests
The authors do not report any conflict of interest or dedicated funding support for this project.
Correspondence
Address correspondence to Amro Ilaiwy, MD, MPA, WakeMed Health & Hospitals, 3024 New Bern Avenue, Suite 301, Raleigh, NC 27610 (ailaiwy@wakemed.org).